

Hemithyroidectomy for low-risk follicular carcinoma of the thyroid: results from a regional hospital
- PMID: 29214321
- PMCID: PMC6024211
- DOI: 10.11622/smedj.2017106
Hemithyroidectomy for low-risk follicular carcinoma of the thyroid: results from a regional hospital
Abstract
Introduction: Excellent outcomes after conservative thyroid surgery for low-risk follicular thyroid carcinoma (FTC) have been reported from highly specialised centres. However, it is uncertain whether low-volume hospitals can achieve similar treatment results.
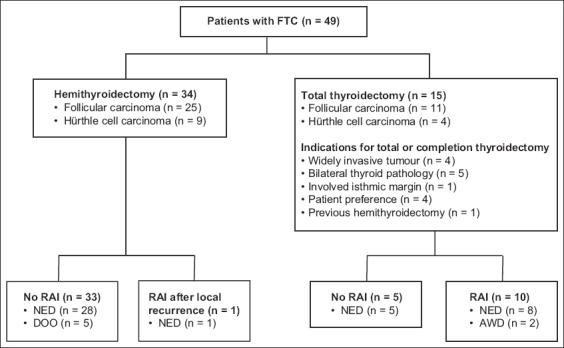
Methods: At our institution, 49 patients with FTC were treated during the period 1991-2014. Patients with minimally invasive FTC (MIFTC) were usually treated with hemithyroidectomy. The demographic data, pathology, treatment modality and oncological outcomes of these patients were retrospectively evaluated.
Results: The tumours were classified as Stage I in 40.8% of patients, Stage II in 32.7%, Stage III in 20.4% and Stage IV in 6.1%, according to the TNM classification system. Only 4 (8.2%) patients had widely invasive FTC (WIFTC). Vascular invasion or capsular invasion alone occurred in 9 (19.1%) and 19 (40.4%) patients, respectively, while 19 (40.4%) patients had simultaneous vascular and capsular invasions. 34 (69.4%) patients with MIFTC initially underwent hemithyroidectomy, while 15 (30.6%) patients underwent total thyroidectomy. Ten patients who underwent total thyroidectomy received radioactive iodine ablation. The mean follow-up duration was 86.9 ± 56.6 months. There was no disease-specific mortality, although two patients with WIFTC remained alive with disease at the end of the study. The five-, ten- and 15-year overall survival rates were 95%, 91% and 84%, respectively. Five patients from the hemithyroidectomy group died due to other illnesses with no evidence of FTC.
Conclusion: Satisfactory disease control and excellent survival for MIFTC is achievable by hemithyroidectomy in community hospitals. Total thyroidectomy should be reserved for WIFTC or aggressive tumours with nodal or distant metastasis.
Keywords: Hürthle cell; follicular thyroid carcinoma; neoplasm metastasis; prognosis; thyroidectomy.
Copyright: © Singapore Medical Association.
Figures
References
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006;295:2164–7. - PubMed
-
- Hedinger CE, Williams ED, Sobin LH. Histological typing of thyroid tumors. In: Hedinger CE, editor. International Histological Classification of Tumors. Berlin: Springer; 1988. pp. 7–68.
-
- Chow SM, Law SC, Mendenhall WM, et al. Follicular thyroid carcinoma:prognostic factors and the role of radioiodine. Cancer. 2002;95:488–98. - PubMed
-
- Huang CC, Hsueh C, Liu FH, Chao TC, Lin JD. Diagnostic and therapeutic strategies for minimally and widely invasive follicular thyroid carcinomas. Surg Oncol. 2011;20:1–6. - PubMed
-
- Thompson LD, Wieneke JA, Paal E, et al. A clinicopathologic study of minimally invasive follicular carcinoma of the thyroid gland with a review of the English literature. Cancer. 2001;91:505–24. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
