

Advances in stereotactic navigation for pelvic surgery
- PMID: 29214516
- PMCID: PMC5956093
- DOI: 10.1007/s00464-017-5968-0
Advances in stereotactic navigation for pelvic surgery
Abstract
Background: Stereotactic navigation could improve the quality of surgery for rectal cancer. Critical challenges related to soft tissue stereotactic pelvic navigation include the potential difference in patient anatomy between intraoperative lithotomy and preoperative supine position for imaging. The objective of this study was to determine the difference in patient anatomy, sacral tilt, and skin fiducial position between these different patient positions and to investigate the feasibility and optimal set-up for stereotactic pelvic navigation.
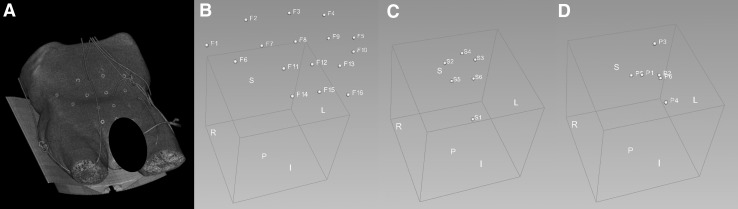
Methods: Four consecutive human anatomical specimens were submitted to repeated CT-scans in a supine and several degrees of lithotomy position. Patient anatomy, sacral tilt, and skin fiducial position were compared by means of an image computing platform. In two specimens, a 10-degree wedge was introduced to reduce the natural tilt of the sacrum during the shift from supine to lithotomy position. A simulation of laparoscopic and transanal surgical procedures was performed to assess the accuracy of the stereotactic navigation.
Results: An up-to-supracentimetric change in patient anatomy was noted between different patient positions. This observation was minimized through the application of a wedge. When switching from supine to another position, sacral retroversion occurred independent of the use of a wedge. There was considerable skin fiducial motion between different positions. Accurate stereotactic navigation was obtained with the least registration error (1.9 mm) when the position of the anatomical specimen was registered in a supine position with straight legs, without pneumoperitoneum, using a conventional CT-scan with an identical specimen positioning.
Conclusion: The change in patient anatomy is small during the sacral tilt induced by positional changes when using a 10-degree wedge, allowing for an accurate stereotactic surgical navigation. This opens up new promising opportunities to increase the quality of surgery for rectal cancer cases where it is difficult or impossible to identify and dissect along the anatomical planes.
Keywords: Anatomy; Computer-assisted; Neuronavigation; Operative; Rectal neoplasms; Stereotaxis techniques; Surgery; Surgical procedures.
Conflict of interest statement
J. Marescaux is president of both IRCAD and IHU Strasbourg, which are partly funded by Karl Storz, Medtronic, and Siemens Healthcare though he has no direct conflict of interest with content discussed in this manuscript. A.G.F. Melani receives remuneration (payment for services not otherwise identified as salary such as consulting fees, honoraria) from Medtronic, Ethicon, Intuitive Surgical, and Verb Surgical though he has no direct conflicts of interest with content discussed in this manuscript. A.R. Wijsmuller, L.G. Romagnolo, V. Agnus, C. Giraudeau, and B. Dallemagne have no conflicts of interest or financial ties to disclose.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
