

Classification of breast cancer in ultrasound imaging using a generic deep learning analysis software: a pilot study
- PMID: 29215311
- PMCID: PMC5965470
- DOI: 10.1259/bjr.20170576
Classification of breast cancer in ultrasound imaging using a generic deep learning analysis software: a pilot study
Abstract
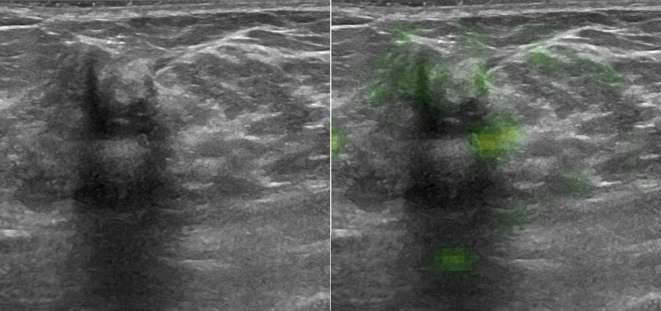
Objective: To train a generic deep learning software (DLS) to classify breast cancer on ultrasound images and to compare its performance to human readers with variable breast imaging experience.
Methods: In this retrospective study, all breast ultrasound examinations from January 1, 2014 to December 31, 2014 at our institution were reviewed. Patients with post-surgical scars, initially indeterminate, or malignant lesions with histological diagnoses or 2-year follow-up were included. The DLS was trained with 70% of the images, and the remaining 30% were used to validate the performance. Three readers with variable expertise also evaluated the validation set (radiologist, resident, medical student). Diagnostic accuracy was assessed with a receiver operating characteristic analysis.
Results: 82 patients with malignant and 550 with benign lesions were included. Time needed for training was 7 min (DLS). Evaluation time for the test data set were 3.7 s (DLS) and 28, 22 and 25 min for human readers (decreasing experience). Receiver operating characteristic analysis revealed non-significant differences (p-values 0.45-0.47) in the area under the curve of 0.84 (DLS), 0.88 (experienced and intermediate readers) and 0.79 (inexperienced reader).
Conclusion: DLS may aid diagnosing cancer on breast ultrasound images with an accuracy comparable to radiologists, and learns better and faster than a human reader with no prior experience. Further clinical trials with dedicated algorithms are warranted. Advances in knowledge: DLS can be trained classify cancer on breast ultrasound images high accuracy even with comparably few training cases. The fast evaluation speed makes real-time image analysis feasible.
Figures







References
-
- Cole-Beuglet C, Beique RA. Continuous ultrasound b-scanning of palpable breast masses. Radiology 1975; 117: 123–8. doi: https://doi.org/10.1148/117.1.123 - DOI - PubMed
-
- Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 2002; 225: 165–75. doi: https://doi.org/10.1148/radiol.2251011667 - DOI - PubMed
-
- Brem RF, Lenihan MJ, Lieberman J, Torrente J. Screening breast ultrasound: past, present, and future. AJR Am J Roentgenol 2015; 204: 234–40. doi: https://doi.org/10.2214/AJR.13.12072 - DOI - PubMed
-
- Giannotti E, Vinnicombe S, Thomson K, McLean D, Purdie C, Jordan L, et al. Shear-wave elastography and greyscale assessment of palpable probably benign masses: is biopsy always required? Br J Radiol 2016; 89: 20150865: 20150865. doi: https://doi.org/10.1259/bjr.20150865 - DOI - PMC - PubMed
-
- Xiao XY, Chen X, Guan XF, Wu H, Qin W, Luo BM. Superb microvascular imaging in diagnosis of breast lesions: a comparative study with contrast-enhanced ultrasonographic microvascular imaging. Br J Radiol 2016; 89: 20160546. doi: https://doi.org/10.1259/bjr.20160546 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
