

Term Elective Induction of Labor and Pregnancy Outcomes Among Obese Women and Their Offspring
- PMID: 29215512
- PMCID: PMC5833989
- DOI: 10.1097/AOG.0000000000002408
Term Elective Induction of Labor and Pregnancy Outcomes Among Obese Women and Their Offspring
Erratum in
-
Term Elective Induction of Labor and Pregnancy Outcomes Among Obese Women and Their Offspring: Correction.Obstet Gynecol. 2018 May;131(5):937. doi: 10.1097/AOG.0000000000002623. Obstet Gynecol. 2018. PMID: 29683900 No abstract available.
Abstract
Objective: To evaluate whether elective induction of labor between 39 through 41 weeks of gestation, as compared with expectant management, is associated with reduced cesarean delivery and other adverse outcomes among obese women and their offspring.
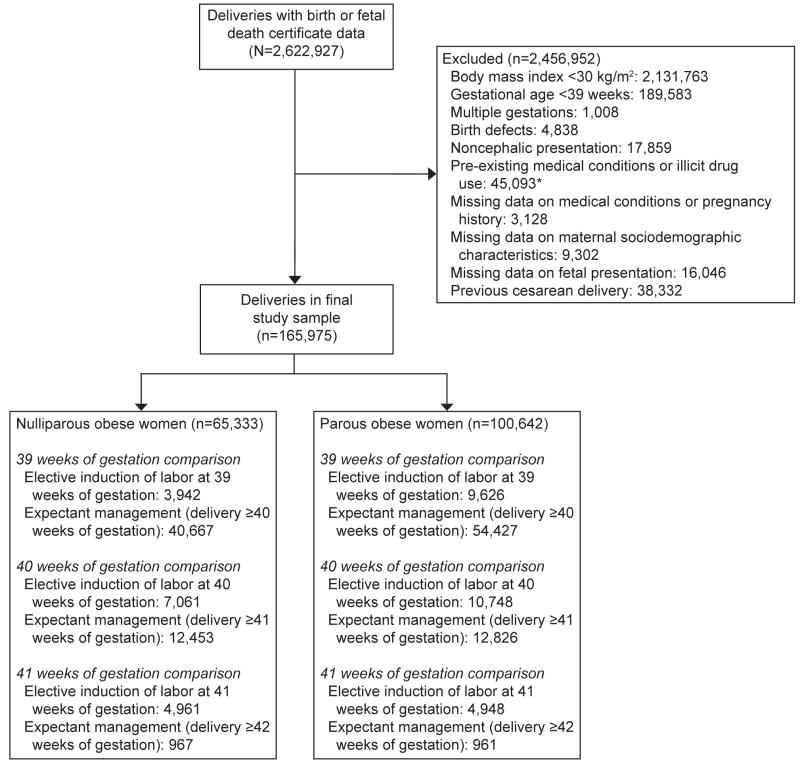
Methods: We conducted a retrospective cohort study using the 2007-2011 California Linked Patient Discharge Data-Birth Cohort File of 165,975 singleton, cephalic, nonanomalous deliveries to obese women. For each gestational week (39-41), we used multivariable logistic regression models, stratified by parity, to assess whether elective induction of labor or expectant management was associated with lower odds of cesarean delivery and other adverse outcomes.
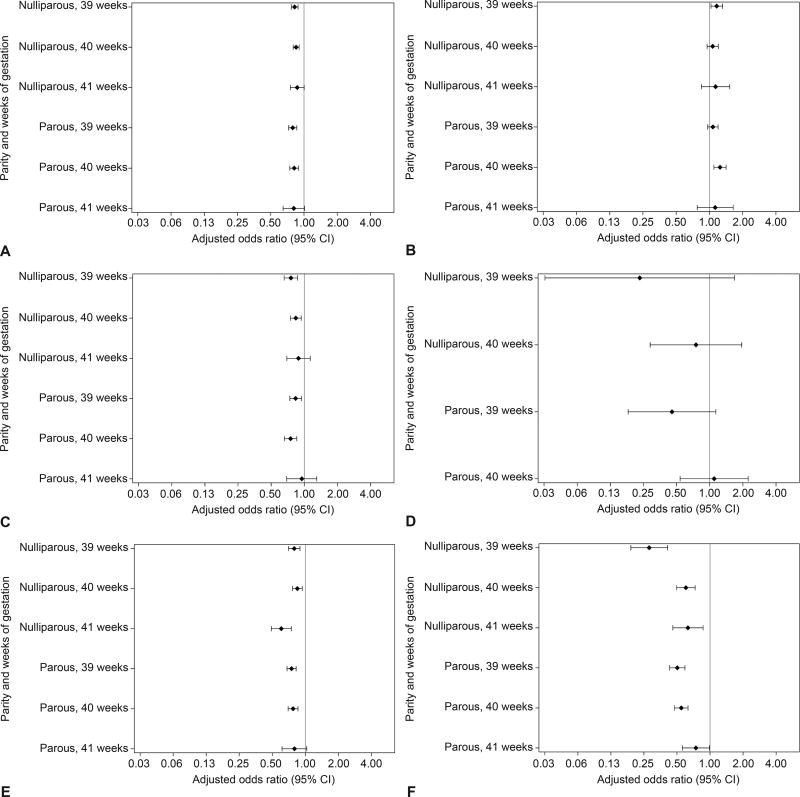
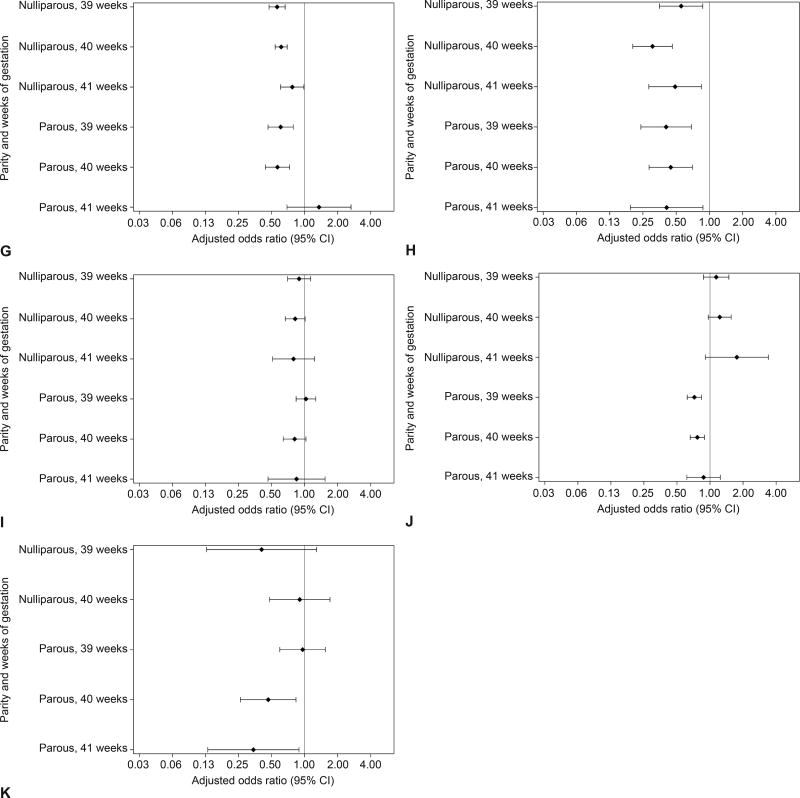
Results: At 39 and 40 weeks of gestation, cesarean delivery was less common in obese nulliparous women who were electively induced compared with those who were expectantly managed (at 39 weeks of gestation, frequencies were 35.9% vs 41.0%, respectively [P<.05]; adjusted odds ratio [OR] 0.82, 95% CI 0.77-0.88). Severe maternal morbidity was less frequent among electively induced obese nulliparous patients (at 39 weeks of gestation, 5.6% vs 7.6% [P<.05]; adjusted OR 0.75, 95% CI 0.65-0.87). Neonatal intensive care unit admission was less common among electively induced obese nulliparous women (at 39 weeks of gestation, 7.9% vs 10.1% [P<.05]; adjusted OR 0.79, 95% CI 0.70-0.89). Patterns were similar among obese parous women at 39 weeks of gestation (crude frequencies and adjusted ORs [95% CIs] were as follows: for cesarean delivery, 7.0% vs 8.7% [P<.05] and 0.79 [0.73-0.86]; for severe maternal morbidity, 3.3% vs 4.0% [P<.05] and 0.83 [0.74-0.94]; for neonatal intensive care unit admission: 5.3% vs 7.4% [P<.05] and 0.75 [0.68-0.82]). Similarly, elective induction at 40 weeks of gestation was associated with reduced odds of cesarean delivery, maternal morbidity, and neonatal intensive care unit admission among both obese nulliparous and parous patients.
Conclusion: Elective labor induction after 39 weeks of gestation was associated with reduced maternal and neonatal morbidity among obese women. Further prospective investigation is necessary.
Conflict of interest statement
The authors did not report any potential conflicts of interest.
Figures
Comment in
-
Term Elective Induction of Labor and Pregnancy Outcomes Among Obese Women and Their Offspring.Obstet Gynecol. 2018 Jun;131(6):1161-1162. doi: 10.1097/AOG.0000000000002658. Obstet Gynecol. 2018. PMID: 29794656 No abstract available.
-
In Reply.Obstet Gynecol. 2018 Jun;131(6):1162. doi: 10.1097/AOG.0000000000002659. Obstet Gynecol. 2018. PMID: 29794657 No abstract available.
-
Elective induction of labour in low risk nulliparous women at term: Caution is needed.Eur J Obstet Gynecol Reprod Biol. 2019 Aug;239:64-66. doi: 10.1016/j.ejogrb.2019.05.037. Epub 2019 Jun 5. Eur J Obstet Gynecol Reprod Biol. 2019. PMID: 31195165
Similar articles
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
Induction of labor before 40 weeks is associated with lower rate of cesarean delivery in women with gestational diabetes mellitus.Am J Obstet Gynecol. 2016 Mar;214(3):364.e1-8. doi: 10.1016/j.ajog.2015.12.021. Am J Obstet Gynecol. 2016. PMID: 26928149
-
Nonmedically indicated induction in morbidly obese women is not associated with an increased risk of cesarean delivery.Am J Obstet Gynecol. 2017 Oct;217(4):451.e1-451.e8. doi: 10.1016/j.ajog.2017.05.048. Epub 2017 May 31. Am J Obstet Gynecol. 2017. PMID: 28578171 Free PMC article.
-
Elective induction of labor at 39 weeks compared with expectant management: a meta-analysis of cohort studies.Am J Obstet Gynecol. 2019 Oct;221(4):304-310. doi: 10.1016/j.ajog.2019.02.046. Epub 2019 Feb 25. Am J Obstet Gynecol. 2019. PMID: 30817905
-
Comparison of Maternal Labor-Related Complications and Neonatal Outcomes Following Elective Induction of Labor at 39 Weeks of Gestation vs Expectant Management: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 May 1;6(5):e2313162. doi: 10.1001/jamanetworkopen.2023.13162. JAMA Netw Open. 2023. PMID: 37171818 Free PMC article.
Cited by
-
Midwifery presence in United States medical centers and labor care and birth outcomes among low-risk nulliparous women: A Consortium on Safe Labor study.Birth. 2019 Sep;46(3):475-486. doi: 10.1111/birt.12407. Epub 2018 Nov 11. Birth. 2019. PMID: 30417436 Free PMC article.
-
Outcomes of Elective Induction of Labor versus Expectant Management among Obese Women at ≥39 Weeks.Am J Perinatol. 2020 Jun;37(7):695-707. doi: 10.1055/s-0039-1688471. Epub 2019 Apr 30. Am J Perinatol. 2020. PMID: 31039597 Free PMC article.
-
Impact of a Policy to Deliver at 39 Weeks for the Indication of Class III Obesity.Obesity (Silver Spring). 2020 Mar;28(3):563-569. doi: 10.1002/oby.22729. Epub 2020 Feb 5. Obesity (Silver Spring). 2020. PMID: 32020789 Free PMC article.
-
Vaginal Dinoprostone Insert versus Cervical Ripening Balloon for Term Induction of Labor in Obese Nulliparas-A Randomized Controlled Trial.J Clin Med. 2022 Apr 11;11(8):2138. doi: 10.3390/jcm11082138. J Clin Med. 2022. PMID: 35456231 Free PMC article.
-
Risk associated with planned mode of delivery in women with obesity: a large population-based retrospective cohort study.Int J Obes (Lond). 2025 May;49(5):835-843. doi: 10.1038/s41366-024-01709-x. Epub 2025 Mar 17. Int J Obes (Lond). 2025. PMID: 40097706 Free PMC article.
References
-
- Aune D, Saugstad OD, Henriksen T, Tonstad S. Maternal body mass index and the risk of fetal death, stillbirth, and infant death: a systematic review and meta-analysis. JAMA. 2014;311(15):1536–46. - PubMed
-
- Sebire NJ, Jolly M, Harris JP, et al. Maternal obesity and pregnancy outcome: a study of 287,213 pregnancies in London. Int J Obes Relat Metab Disord. 2001;25(8):1175–82. - PubMed
-
- Branum A, Kirmeyer S, Gregory E. Prepregnancy Body Mass Index by Maternal Characteristics and State: Data From the Birth Certicate, 2014. Natl Vital Stat Rep. 2016;65(6):1–11. - PubMed
-
- Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol. 2004;103(2):219–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
