

De novo and secondary anaplastic meningiomas: a study of clinical and histomolecular prognostic factors
- PMID: 29216385
- PMCID: PMC6280137
- DOI: 10.1093/neuonc/nox231
De novo and secondary anaplastic meningiomas: a study of clinical and histomolecular prognostic factors
Abstract
Background: Following recent studies underlining the differences between de novo and secondary anaplastic meningiomas and the prognostic value of telomerase reverse transcriptase (TERT) promoter mutation, we decided to conduct a multicenter retrospective study to address these questions and determine specific prognostic factors in each of these 2 anaplastic meningioma subgroups.
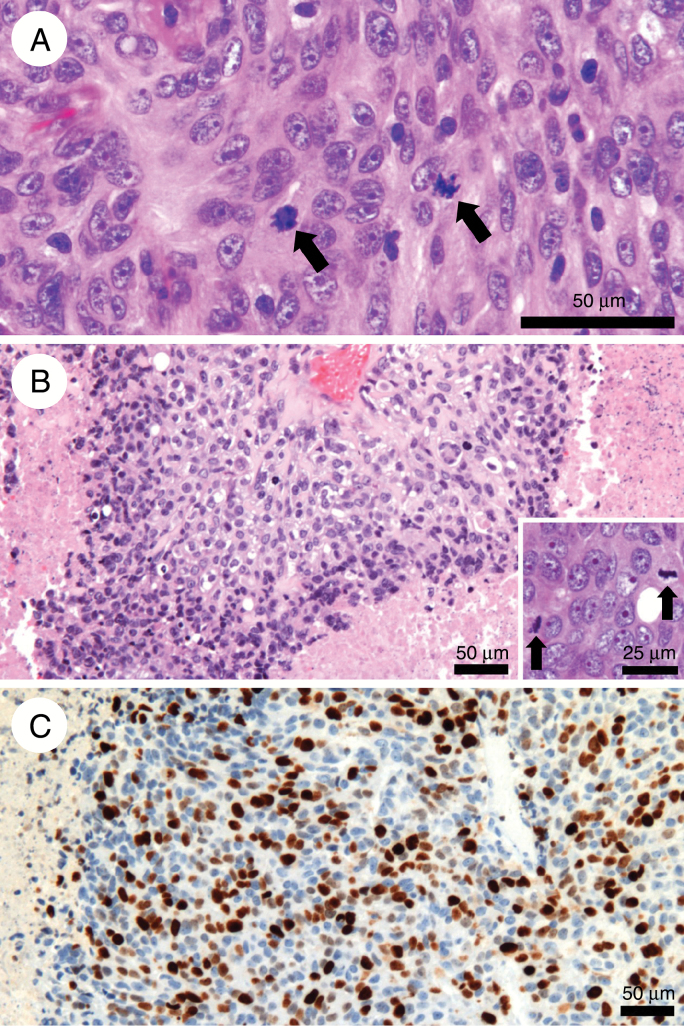
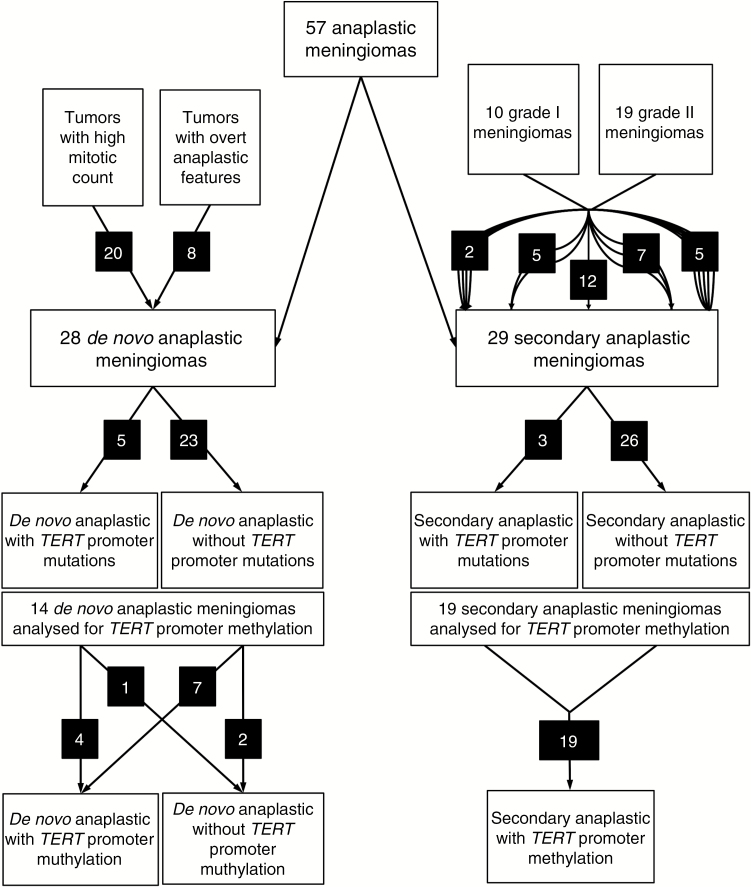
Methods: Among the 68 meningioma cases initially selected, only 57 were confirmed as anaplastic meningiomas after centralized pathological review. TERT promoter mutation analysis was performed in all cases.
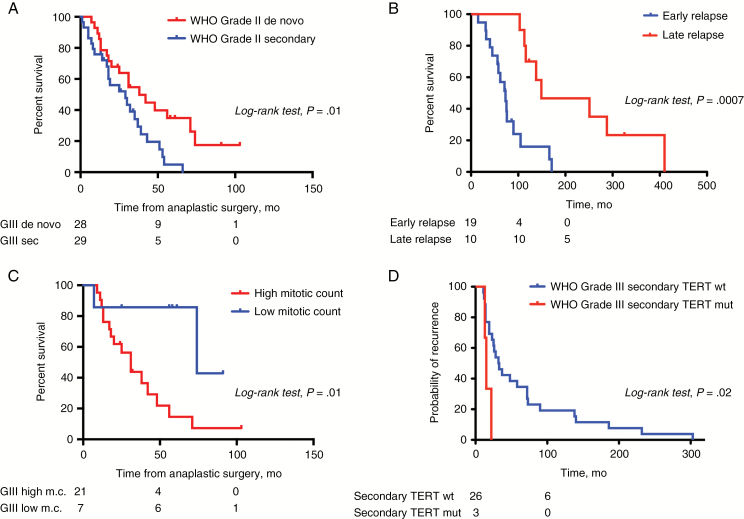
Results: Median overall survival was 2.6 years and 5-year survival rate was 10%. This study confirmed the better prognosis of de novo anaplastic meningiomas (28 tumors) compared with secondary anaplastic meningiomas (29 tumors) (P = 0.02). In the "de novo" group, meningiomas diagnosed on histological anaplasia alone had a better prognosis than those in patients with a high number of mitoses with or without anaplasia (P = 0.01). In the "secondary" group, tumors demonstrate very heterogeneous clinical courses leading to malignant transformation, and time to first relapse as a low-grade tumor was a strong predictor of overall survival (P = 0.0007). TERT promoter mutation in anaplastic meningiomas was rare (14%) and did not influence overall survival but was associated with a shorter recurrence-free survival in the secondary anaplastic meningioma subgroup (P = 0.02). The absence of TERT promoter methylation, although rare (3/33 cases), may be associated with prolonged overall survival (P = 0.02).
Conclusion: This study highlights the different prognoses of de novo and secondary anaplastic meningiomas with specific prognostic factors in each subgroup. The analysis of TERT mutation and methylation could provide additional prognostic insights.
Figures
Comment in
-
De novo and secondary anaplastic meningiomas: natural history, prognosis, and the TERT promoter.Neuro Oncol. 2018 Jul 5;20(8):1009-1010. doi: 10.1093/neuonc/noy101. Neuro Oncol. 2018. PMID: 29982653 Free PMC article. No abstract available.
References
-
- Aghi MK, Carter BS, Cosgrove GR et al. Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery. 2009;64(1):56–60; discussion 60. - PubMed
-
- Aizer AA, Bi WL, Kandola MS et al. Extent of resection and overall survival for patients with atypical and malignant meningioma: extent of resection and recurrence in meningioma. Cancer. 2015;121(24):4376–4381. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
