

Use of a hydrophilic coating wire reduces significantly the rate of central vein punctures and the incidence of pneumothorax in totally implantable access port (TIAP) surgery
- PMID: 29216858
- PMCID: PMC5721482
- DOI: 10.1186/s12893-017-0329-4
Use of a hydrophilic coating wire reduces significantly the rate of central vein punctures and the incidence of pneumothorax in totally implantable access port (TIAP) surgery
Abstract
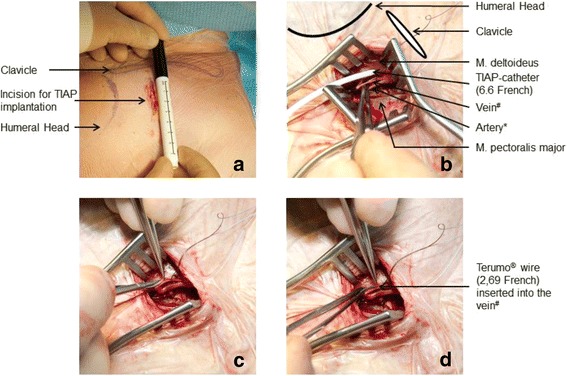
Background: Insertion of a Totally Implantable Access Port (TIAP) can be performed either via Central Vein Puncture (CVP) or Brachiocephalic Vein Cut-down (venous section-VS). The primary success rate of TIAP implantation using VS rarely ever achieves 100%. The objective of this study was to describe a modified VS approach using a hydrophilic coated wire (TVS).
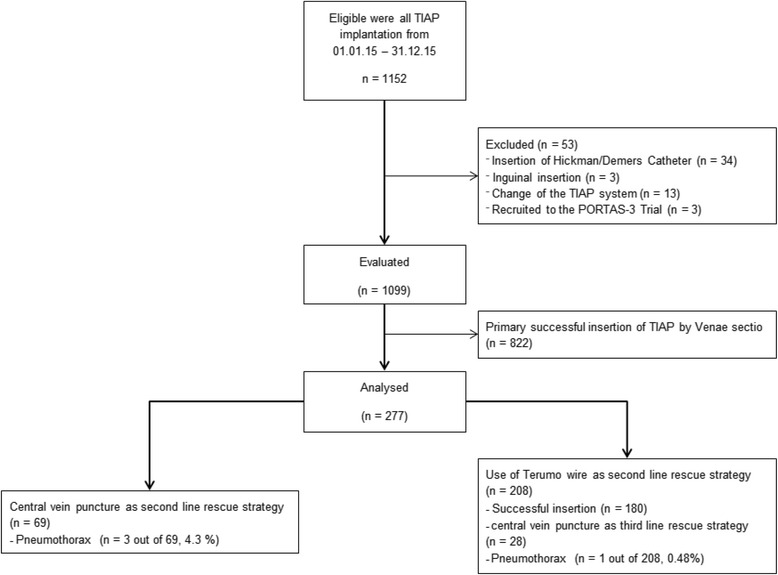
Methods: From 01.01.2015 to 31.12.2015, all patients receiving TIAP implantations were screened. During this time, all patients in whom the primary VS procedure was found to be unsuccessful were analysed.
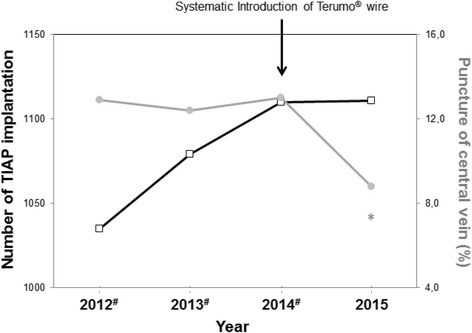
Results: In 2015, 1152 patients had TIAP implantations performed by 24 different surgeons. Of these, 277 patients needed a second line rescue strategy either by CVP (n = 69) or TVS (n = 208). There were no statistically significant differences regarding demographics or indication for TIAP implantation between CVP and TVS. The operation time and the qualification of the operating surgeon between CVP and TVS did not differ significantly. After the introduction of the guidewire with a hydrophilic coated wire, the need for CVP decreased significantly from 12.7% to 8.8% (p < 0.0001). In patients receiving CVP as a second line rescue strategy, the incidence of pneumothorax (n = 3 patients (4.3%)) was significantly higher compared to patients with TVS as a second line rescue strategy (n = 1 patient (0.48%), p = 0.02).
Conclusion: The use of a hydrophilic coated wire significantly decreased the number of CVP and the incidence of pneumothorax. TVS is a safe and successful second-line rescue strategy.
Background: Insertion of a Totally Implantable Access Port (TIAP) can be performed either via Central Vein Puncture (CVP) or Brachiocephalic Vein Cut-down (venous section-VS). The primary success rate of TIAP implantation using VS rarely ever achieves 100%. The objective of this study was to describe a modified VS approach using a hydrophilic coated wire (TVS).
Methods: From 01.01.2015 to 31.12.2015, all patients receiving TIAP implantations were screened. During this time, all patients in whom the primary VS procedure was found to be unsuccessful were analysed.
Results: In 2015, 1152 patients had TIAP implantations performed by 24 different surgeons. Of these, 277 patients needed a second line rescue strategy either by CVP (n = 69) or TVS (n = 208). There were no statistically significant differences regarding demographics or indication for TIAP implantation between CVP and TVS. The operation time and the qualification of the operating surgeon between CVP and TVS did not differ significantly. After the introduction of the guidewire with a hydrophilic coated wire, the need for CVP decreased significantly from 12.7% to 8.8% (p < 0.0001). In patients receiving CVP as a second line rescue strategy, the incidence of pneumothorax (n = 3 patients (4.3%)) was significantly higher compared to patients with TVS as a second line rescue strategy (n = 1 patient (0.48%), p = 0.02).
Conclusion: The use of a hydrophilic coated wire significantly decreased the number of CVP and the incidence of pneumothorax. TVS is a safe and successful second-line rescue strategy.
Keywords: Guide wire; Pneumothorax; Totally implantable access port; Venous cut-down.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective study was approved by the local ethics committee of the University of Heidelberg (S-584/2016).
Consent for publication
Not applicable
Competing interests
The authors declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Niederhuber JE, et al. Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery. 1982;92(4):706–712. - PubMed
-
- Rotzinger R, et al. Placement of central venous port catheters and peripherally inserted central catheters in the routine clinical setting of a radiology department: analysis of costs and intervention duration learning curve. Acta Radiol. 2017:284185117695664. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
