

Effect of Orthokeratology on myopia progression: twelve-year results of a retrospective cohort study
- PMID: 29216865
- PMCID: PMC5721542
- DOI: 10.1186/s12886-017-0639-4
Effect of Orthokeratology on myopia progression: twelve-year results of a retrospective cohort study
Abstract
Background: Several studies reported the efficacy of orthokeratology for myopia control. Somehow, there is limited publication with follow-up longer than 3 years. This study aims to research whether overnight orthokeratology influences the progression rate of the manifest refractive error of myopic children in a longer follow-up period (up to 12 years). And if changes in progression rate are found, to investigate the relationship between refractive changes and different baseline factors, including refraction error, wearing age and lens replacement frequency. In addition, this study collects long-term safety profile of overnight orthokeratology.
Methods: This is a retrospective study of sixty-six school-age children who received overnight orthokeratology correction between January 1998 and December 2013. Thirty-six subjects whose baseline age and refractive error matched with those in the orthokeratology group were selected to form control group. These subjects were followed up at least for 12 months. Manifest refractions, cycloplegic refractions, uncorrected and best-corrected visual acuities, power vector of astigmatism, corneal curvature, and lens replacement frequency were obtained for analysis.
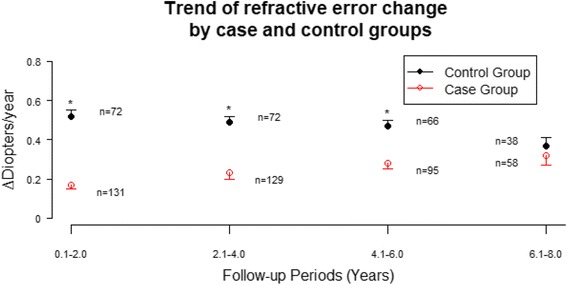
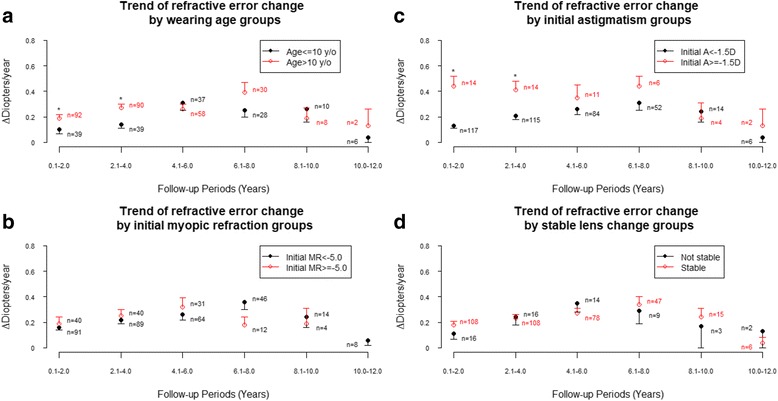
Results: Data of 203 eyes were derived from 66 orthokeratology subjects (31 males and 35 females) and 36 control subjects (22 males and 14 females) enrolled in this study. Their wearing ages ranged from 7 years to 16 years (mean ± SE, 11.72 ± 0.18 years). The follow-up time ranged from 1 year to 13 years (mean ± SE, 6.32 ± 0.15 years). At baseline, their myopia ranged from -0.5 D to -8.0 D (mean ± SE, -3.70 ± 0.12 D), and astigmatism ranged from 0 D to -3.0 D (mean ± SE, -0.55 ± 0.05 D). Comparing with control group, orthokeratology group had a significantly (p < 0.001) lower trend of refractive error change during the follow-up periods. According to the analysis results of GEE model, greater power of astigmatism was found to be associated with increased change of refractive error during follow-up years.
Conclusions: Overnight orthokeratology was effective in slowing myopia progression over a twelve-year follow-up period and demonstrated a clinically acceptable safety profile. Initial higher astigmatism power was found to be associated with increased change of refractive error during follow-up years.
Keywords: Contact lenses; Myopia; Myopia control; Optical intervention; Orthokeratology.
Conflict of interest statement
Ethics approval and consent to participate
This study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Institutional Ethical Committee Review Board of Buddhist Tzu Chi General Hospital, Hualien, Taiwan (REC No.: IRB103–17-B).
We confirmed that all written consents were obtained from participants. For those participants under the age of 16, the consent forms were signed by the parents on behalf of those participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
