

Socio-demographic determinants and effect of structured personal diabetes care: a 19-year follow-up of the randomized controlled study diabetes Care in General Practice (DCGP)
- PMID: 29216868
- PMCID: PMC5721594
- DOI: 10.1186/s12902-017-0227-x
Socio-demographic determinants and effect of structured personal diabetes care: a 19-year follow-up of the randomized controlled study diabetes Care in General Practice (DCGP)
Abstract
Background: We investigated how four aspects of socio-demography influence the effectiveness of an intervention with structured personal diabetes care on long-term outcomes.
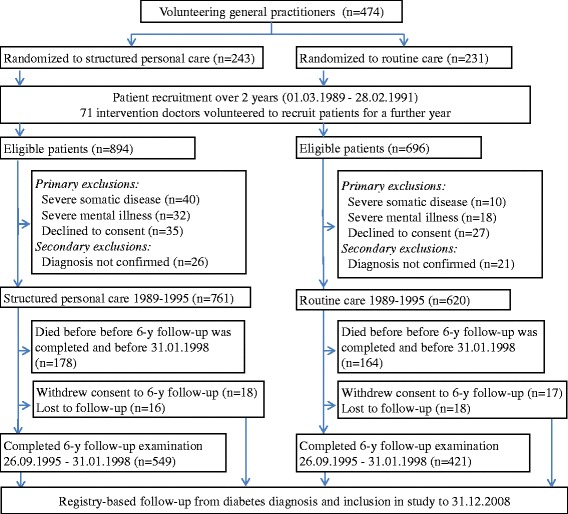
Methods: The Diabetes Care in General Practice (DCGP) study is a cluster-randomized trial involving a population-based sample of 1381 patients with newly diagnosed type 2-diabetes mellitus. We investigated how education, employment, cohabitation status and residence influenced the effectiveness of 6 years of intervention with structured personal diabetes care, resembling present day recommendations. Outcomes were incidence of any diabetes-related endpoint and death during 19 years after diagnosis, and cardiovascular risk factors, behaviour, attitudes and process-of-care variables 6 years after diagnosis.
Results: Structured personal care reduced the risk of any diabetes-related endpoint and the effect of the intervention was modified by geographical area (interaction p = 0.034) with HR of 0.71 (95%CI: 0.60-0.85) and of 1.07 (95%CI: 0.77-1.48), for patients in urban and rural areas, respectively. Otherwise, there was no effect modification of education, employment and civil status on the intervention for the final endpoints. There were no noticeable socio-demographic differences in the effect of the intervention on cardiovascular risk factors, behaviour, attitudes, and process-of-care.
Conclusion: Structured personal care reduced the aggregate outcome of any diabetes-related endpoint and independent of socio-demographic factors similar effect on cardiovascular risk factors, behaviour, attitudes and process of care, but the intervention did not change the existing inequity in mortality and morbidity. Residence modified the uptake of the intervention with patients living in urban areas having more to gain of the intervention than rural patients, further investigations is warranted.
Trial registration: ClinicalTrials.gov registration no. NCT01074762 (February 24, 2010).
Keywords: Clinical outcomes; Intervention; Social inequalities; Type 2 diabetes mellitus.
Conflict of interest statement
Ethics approval and consent to participate
All patients gave verbal informed consent to participate, following a dialogue with their GP, where the patients could ask questions, to secure an informed consent. The Ethics Committee of Copenhagen and Frederiksberg (V.100.869/87) approved the study and this procedure for informed consent. When the study started off in 1988 it was coutume to seek informed consent orally.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Walker J, Halbesma N, Lone N, McAllister D, Weir CJ, Wild SH. Scottish diabetes research network epidemiology G: socioeconomic status, comorbidity and mortality in patients with type 2 diabetes mellitus in Scotland 2004-2011: a cohort study. J Epidemiol Community Health. 2016;70(6):596–601. doi: 10.1136/jech-2015-206702. - DOI - PMC - PubMed
-
- Dagenais GR, Gerstein HC, Zhang X, McQueen M, Lear S, Lopez-Jaramillo P, Mohan V, Mony P, Gupta R, Kutty VR, et al. Variations in diabetes prevalence in low-, middle-, and high-income countries: results from the prospective urban and rural epidemiological study. Diabetes Care. 2016;39(5):780–787. doi: 10.2337/dc15-2338. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
