

Characteristics and Performance of Unilateral Kidney Transplants from Deceased Donors
- PMID: 29217537
- PMCID: PMC5753314
- DOI: 10.2215/CJN.06550617
Characteristics and Performance of Unilateral Kidney Transplants from Deceased Donors
Abstract
Background and objectives: The fraction of kidneys procured for transplant that are discarded is rising in the United States. Identifying donors from whom only one kidney was discarded allows us to control for donor traits and better assess reasons for organ discard.
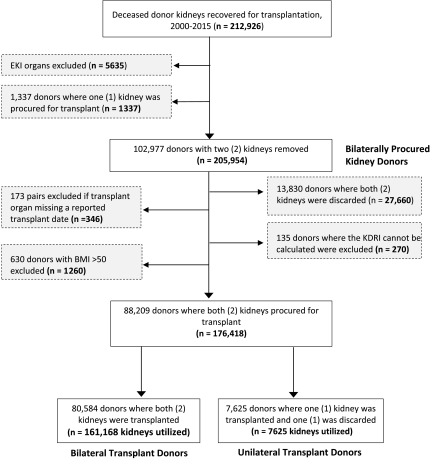
Design, setting, participants, & measurements: We conducted a retrospective cohort study using United Network for Organ Sharing Standard Transplant Analysis and Research file data to identify deceased donors from whom two kidneys were procured and at least one was transplanted. Unilateral pairs were defined as kidney pairs from a single donor from whom one kidney was discarded ("unilateral discard") but the other was transplanted ("unilateral transplant"). Organ quality was estimated using the Kidney Donor Risk Index and Kidney Donor Profile Index (KDPI). We compared all-cause graft failure rates for unilateral transplants to those for bilateral transplant Kaplan-Meier methods, and life table methodology was used to evaluate 1-, 2-, 3-, and 5-year survival rates of transplants from bilateral and unilateral donors.
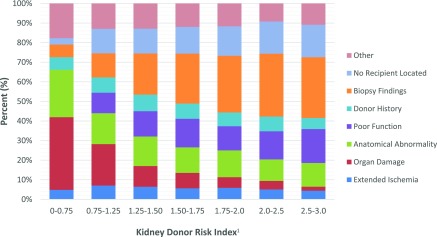
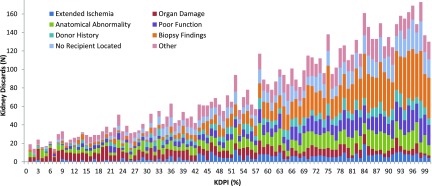
Results: Compared with bilateral donors (i.e., both kidneys transplanted) (n=80,584), unilateral donors (i.e., only one kidney transplanted) (n=7625) had higher mean terminal creatinine (1.3±2.1 mg/dl versus 1.1±0.9 mg/dl) and KDPI (67%±25% versus 42%±27%), were older, and were more likely to have hypertension, diabetes, hepatitis C, terminal stroke, or meet Centers for Disease Control and Prevention high-risk donor criteria. Unilateral discards were primarily attributed to factors expected to be similar in both kidneys from a donor: biopsy findings (22%), no interested recipient (13%), and donor history (7%). Anatomic abnormalities (14%), organ damage (11%), and extended ischemia (6%) accounted for about 30% of discards, but were the commonest reasons among low KDPI kidneys. Among kidneys with KDPI≥60%, there was an incremental difference in allograft survival over time (for unilateral versus bilateral transplants, 1-year survival: 83% versus 87%; 3-year survival: 69% versus 73%; 5-year survival: 51% versus 58%).
Conclusions: A large number of discarded kidneys were procured from donors whose contralateral kidneys were transplanted with good post-transplant outcomes.
Keywords: Allografts; Biopsy; Centers for Disease Control and Prevention (U.S.); Death; Hepatitis C; Life Tables; Retrospective Studies; Stroke; Survival Rate; Tissue Donors; United States; cadaver organ transplantation; clinical epidemiology; creatinine; diabetes mellitus; hypertension; kidney; kidney transplantation; transplant outcomes.
Copyright © 2018 by the American Society of Nephrology.
Figures
Comment in
-
Compelling Evidence of the Need for Policy Change to Decrease Deceased Donor Kidney Discard in the United States: Waste Not Want Less.Clin J Am Soc Nephrol. 2018 Jan 6;13(1):13-15. doi: 10.2215/CJN.12671117. Epub 2017 Dec 7. Clin J Am Soc Nephrol. 2018. PMID: 29217538 Free PMC article. No abstract available.
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- Rabbat CG, Thorpe KE, Russell JD, Churchill DN: Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol 11: 917–922, 2000 - PubMed
-
- Oniscu GC, Brown H, Forsythe JL: Impact of cadaveric renal transplantation on survival in patients listed for transplantation. J Am Soc Nephrol 16: 1859–1865, 2005 - PubMed
-
- Merion RM, Ashby VB, Wolfe RA, Distant DA, Hulbert-Shearon TE, Metzger RA, Ojo AO, Port FK: Deceased-donor characteristics and the survival benefit of kidney transplantation. JAMA 294: 2726–2733, 2005 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
