

doi: 10.3324/haematol.2017.174987.
Epub 2017 Dec 7.
High throughput sequencing in acute lymphoblastic leukemia reveals clonal architecture of central nervous system and bone marrow compartments
Affiliations
- PMID: 29217777
- PMCID: PMC5830395
- DOI: 10.3324/haematol.2017.174987
Item in Clipboard
High throughput sequencing in acute lymphoblastic leukemia reveals clonal architecture of central nervous system and bone marrow compartments
Haematologica.
2018 Mar.
No abstract available
Figures
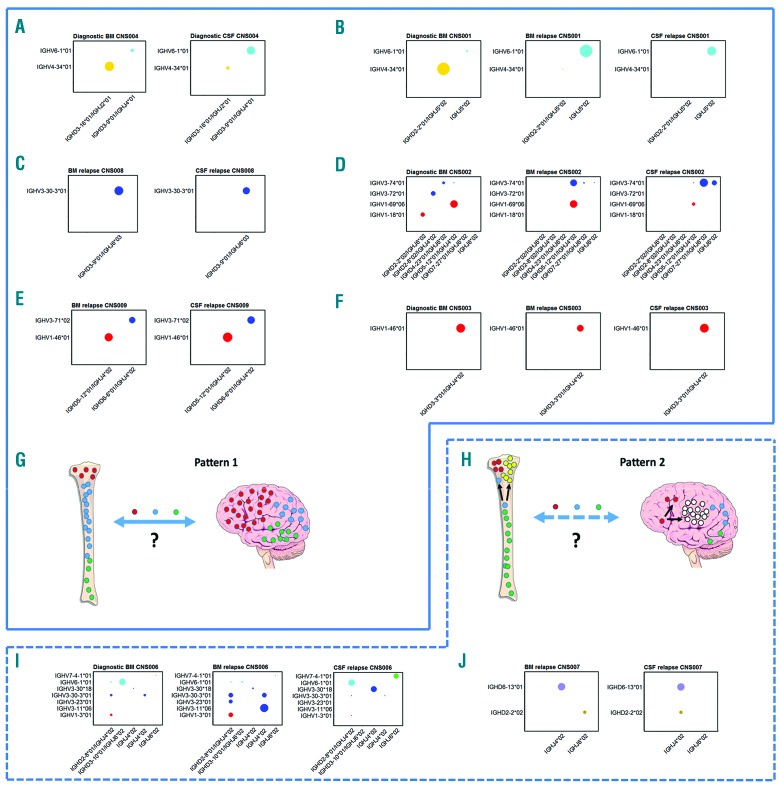
Combined relapses, CNS disease at presentation and schematic presentation of the types of relapse seen. (A) CNS004. CNS involvement at diagnosis, showing that both compartments share the two dominant clones, albeit at reversed frequencies. (B) CNS001. The dominant diagnostic BM clone is IGHV4-34*01/IGHD2-2*01/IGHJ5*02 at 85%; present at 0.002% in BM relapse and undetectable at CNS relapse. The dominant clone in BM and CNS relapse samples is IGHV6-1*01/IGHJ5*02 at 78% and 88%, respectively (only 4% in original diagnostic BM). (C) CNS008. The identical dominant clone IGHV3-30-3*01/IGHD3-9*01/IGHJ6*03 at 95% and 64% in BM relapse and CNS relapse, respectively. (D) CNS002. The dominant diagnostic BM clones are 36% IGHV1-69*06/IGHD5-12*01/IGHJ4*02, 11% IGHV3-72*01/IGHD2-8*02/IGHJ4*02 and 10% IGHV1-18*01/IGHD2-2*02/IGHJ6*02. The dominant clone in the relapse BM sample is also IGHV1-69*06/IGHD5-12*01/IGHJ4*02 at 45%, however, this is only present at 5% in the CNS relapse sample. The second dominant clone in the relapse BM sample, IGHV3-74*01/IGHD5-12*01/IGHJ4*02 at 34%, is only present at 0.1% in diagnostic BM and 0.1% in CNS relapse. The CNS relapse dominant clone is IGHV3-74*01/IGHD7-27*01/IGHJ6*02 at 43%, which is absent in the original diagnostic BM, and only 0.6% in BM relapse. The second dominant clone in the CNS is IGHV3-74*01/IGHJ6*02 at 14% (which is again absent in the original diagnostic, and only 0.06% in BM relapse). The dominant clones in the CNS (IGHV3-74*01/IGHD7-27*01/IGHJ6*02 and IGHV3-74*01/IGHJ6*02) share the same IGHV and IGHJ gene usage, but the CDR3 regions are different and unrelated, as illustrated in Online Supplementary Figure S1. (E) CNS009. The identical dominant clones IGHV1-46*01/IGHD5-12*01/IGHJ4*02 at 34% and 48%, and IGHV3-71*02/IGHD6-6*01/IGHJ4*02 at 31% and 40% in BM and CNS, respectively. (F) CNS003. The dominant clone in all three samples is IGHV1-46*01/IGHD3-3*01/IGHJ4*02 at 91%, 50% and 94% in diagnosis BM, BM relapse and CNS relapse, respectively. (G and H) Schematic presentation of the two patterns of relapse seen. Left panel (“Pattern 1”) shows the same ALL clones in BM and CNS at relapse with no evidence for selection of “CNS-tropic” subclones, which could be due to relapse occurring at one or other site and then free trafficking between the CNS and BM, or to the same clones surviving treatment independently at the two sites. The right panel (“Pattern 2”) shows the alternative pattern, where there is evidence for some separate clonal evolution at the two sites, although many clones are also present in both compartments. (I) CNS006. Shows change in dominant clones from diagnosis through to combined BM and CNS relapse. The dominant diagnostic BM clone is IGHV6-1*01/IGHD3-10*01/IGHJ6*02 26% (this is at a very low level of 0.9% in relapse BM, and undetectable in CNS relapse). IGHV3-30-3*01/IGHJ4*02 was only 2% at diagnosis but 10% in relapse BM and 1% in CNS relapse. The dominant clone in the relapse BM, IGHV3-11*06/IGHJ4*02 at 41% was not detectable in the diagnostic sample or in CNS relapse samples. Other dominant relapse BM clones were 11% IGHV1-3*01/IGHD2-8*01/IGHJ4*02 (2% in original diagnostic BM and 1% in CNS relapse), and 10% IGHV3-30-3*01/IGHD2-8*01/IGHJ4*02 (2% in original diagnostic BM and 1% in CNS relapse). The dominant clone in CNS relapse, IGHV6-1*01/IGHD2-8*01/IGHJ4*02 at 26% was only low level in original diagnostic and relapse BM samples at 0.4% and 0.5%, respectively. The other dominant clones in the CNS were 21% IGHV3-30*18/IGHJ4*02 (0.01% in original diagnostic and relapse BM, respectively) and 16% IGHV7-4-1*01/IGHJ6*02 (0.02% in original diagnostic and 0.1% in relapse BM). (J) CNS007. The identical dominant clone IGHD6-13*01/IGHJ4*02 at 37% and 45% in the BM relapse and CNS relapse samples, respectively. However there is a smaller clone (15%) IGHD2-2*02/IGHJ4*02 in BM, not detectable in the CNS sample. In contrast, there is 11% IGHD2-2*02/IGHJ4*02 in CNS relapse not detectable in the BM relapse sample. CSF: cerebrospinal fluid; BM: bone marrow.
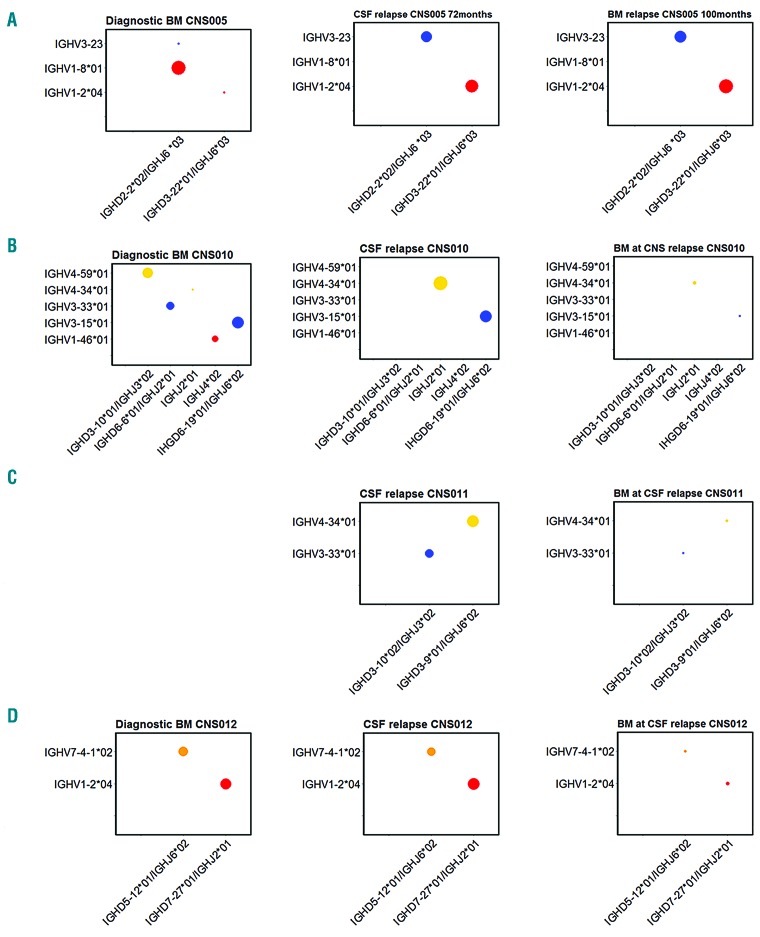
Isolated CNS relapses. (A) CNS005. The dominant diagnostic BM clone is IGHV1-8*01/IGHD2-2*02/IGHJ6*03 at 55%. At relapse, the dominant clones are IGHV3-23/IGHD2-2*02/IGHJ6*03 and IGHV1-2*04/IGHD3-22*01/IGHJ6*03 at 40% and 48% in BM, and 39% and 45% in CNS, respectively. In original diagnostic BM, IGHV3-23/IGHD2-2*02/IGHJ6*03 represents 0.005% and IGHV1-2*04/IGHD3-22*01/IGHJ6*03 represents 0.01%. The dominant clone in the diagnostic BM, IGHV1-8*01/IGHD2-2*02/IGHJ6*03 at 55% is not detectable at relapse, but further analysis showed that this has been V-V replaced, whereby IGHV1-8*01 was replaced to create the IGHV3-23/IGHD2-2*02/IGHJ6*03 clone at relapse (Online Supplementary Figure S2). The presence of the IGHV3-23/IGHD2-2*02/IGHJ6*03 clone in diagnostic BM, albeit at a very low level, also demonstrates there is V-V replacement at diagnosis. (B) CNS010. The dominant clone in diagnostic BM is IGHV3-15*01/IGHD6-19*01/IGHJ6*02 at 31%. There are three other subclones, 24% IGHV4-59*01/IGHD3-10*01/IGHJH3*02, 12% IGHV3-33*01/IGHD6-6*01/IGHJ2*01 and 6% IGHV1-46*01/IGHJ4*02. At time of CNS relapse, the dominant clone is also IGHV3-15*01/IGHD6-19*01/IGHJ6*02 at 41%, however, the three other dominant clones present in diagnostic BM are undetectable in the CSF sample. The other dominant clone in CNS relapse is IGHV4-59*01/IGHD3-10*01/IGHJH3*02 at 46%, which is only present at a level of 0.0001% in diagnostic BM. The BM in morphological remission at time of CNS relapse shows a very low level of the CNS dominant clone IGHV4-34*01/IGHJ2*01 at a level of 0.12%, likewise the original diagnostic BM clone IGHV3-15*01/IGHD6-19*01/IGHJ6*02 at 0.05%. (C) CNS011. The dominant clones in CSF at CNS relapse; IGHV4-34/IGHD3-9*01/IGHJ6*02 at 54% and IGHV3-33*01/IGHD3-10*02/IGHJ3*02 at 34%. These clones are detected at a low level of 0.54% and 0.33%, respectively, in BM at time of CNS relapse, with no additional dominant clones detected. (D) CNS012. The dominant clones in diagnostic BM are IGHV1-2*04/IGHD7-27*01/IGHJ2*01 and IGHV7-4-1*02/IGHD5-12*01/IGHJ6*02 at 32.4% and 31.7%, respectively. In the CNS relapse CSF sample, the same two dominant clones are present at comparable levels. The BM at time of CNS relapse was morphologically negative, however, there was low-level positivity for both clones by both real-time PCR and HTS. CSF: cerebrospinal fluid; BM: bone marrow.
References
-
- Frishman-Levy L, Izraeli S. Advances in understanding the pathogenesis of CNS acute lymphoblastic leukaemia and potential for therapy. Br J Haematol. 2017;176(2):157–167. - PubMed
-
- van der Velden VH, de Launaij D, de Vries JF, et al. New cellular markers at diagnosis are associated with isolated central nervous system relapse in paediatric B-cell precursor acute lymphoblastic leukaemia. Br J Haematol. 2016;172(5):769–781. - PubMed
-
- Levinsen M, Marquart HV, Groth-Pedersen L, et al. Leukemic blasts are present at low levels in spinal fluid in one-third of childhood acute lymphoblastic leukemia cases. Pediatr Blood Cancer. 2016;63(11):1935–1942. - PubMed
-
- Pui CH, Howard SC. Current management and challenges of malignant disease in the CNS in paediatric leukaemia. Lancet Oncol. 2008;9(3):257–268. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
