

Rational management approach to pure red cell aplasia
- PMID: 29217782
- PMCID: PMC5792266
- DOI: 10.3324/haematol.2017.175810
Rational management approach to pure red cell aplasia
Abstract
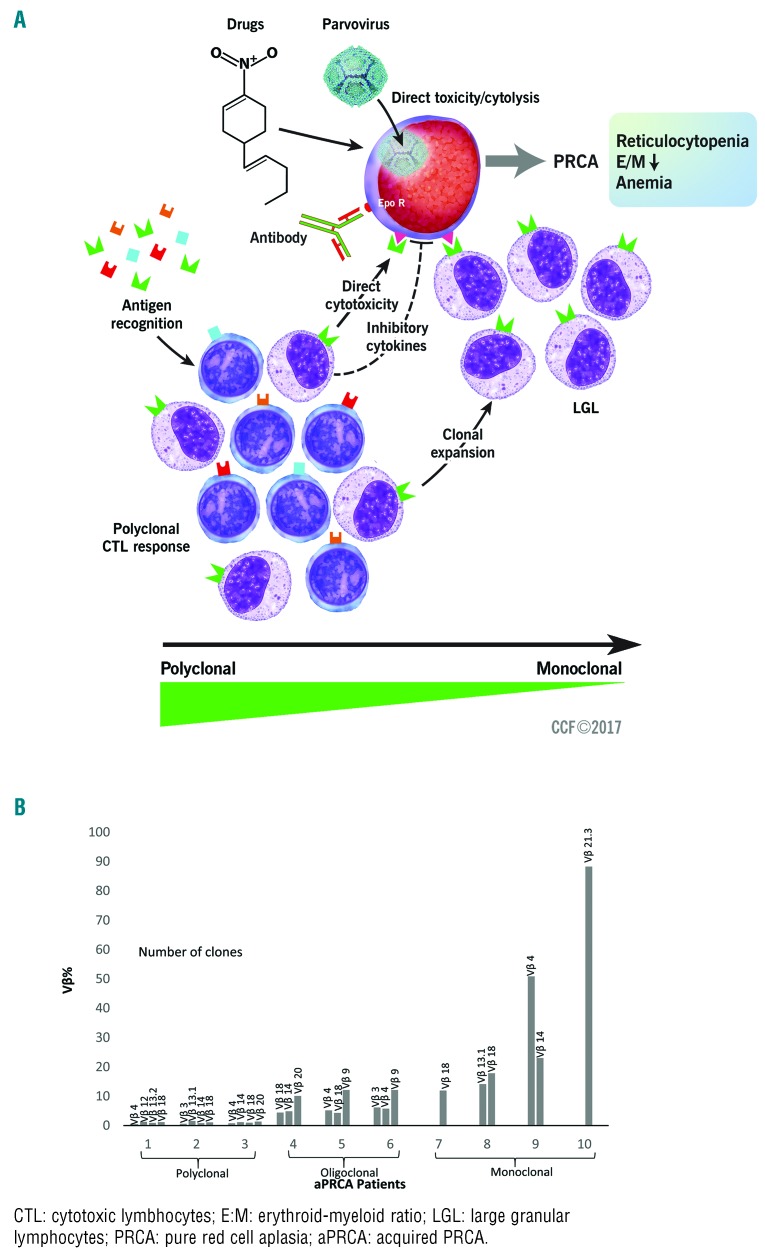
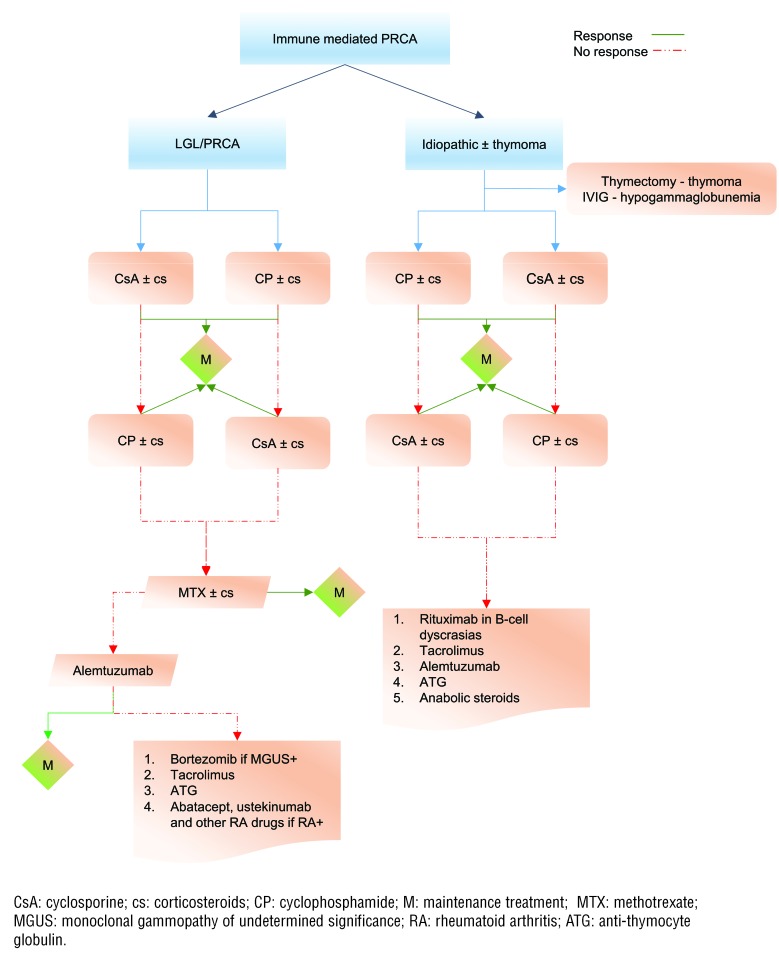
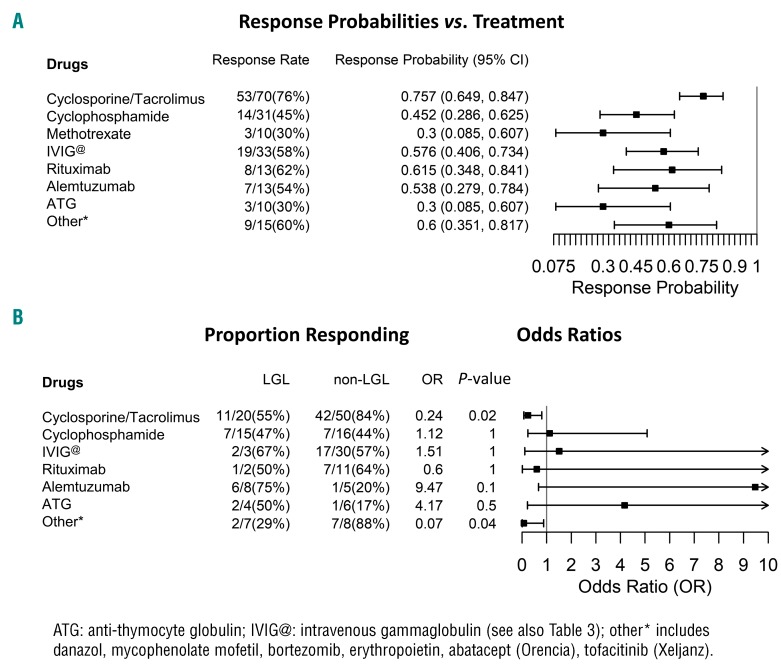
Pure red cell aplasia is an orphan disease, and as such lacks rationally established standard therapies. Most cases are idiopathic; a subset is antibody-mediated. There is overlap between idiopathic cases and those with T-cell large granular lymphocytic leukemia, hypogammaglobulinemia, and low-grade lymphomas. In each of the aforementioned, the pathogenetic mechanisms may involve autoreactive cytotoxic responses. We selected 62 uniformly diagnosed pure red cell aplasia patients and analyzed their pathophysiologic features and responsiveness to rationally applied first-line and salvage therapies in order to propose diagnostic and therapeutic algorithms that may be helpful in guiding the management of prospective patients, 52% of whom were idiopathic, while the others involved large granular lymphocytic leukemia, thymoma, and B-cell dyscrasia. T-cell-mediated responses ranged between a continuum from polyclonal to monoclonal (as seen in large granular lymphocytic leukemia). During a median observation period of 40 months, patients received a median of two different therapies to achieve remission. Frequently used therapy included calcineurin-inhibitors with a steroid taper yielding a first-line overall response rate of 76% (53/70). Oral cyclophosphamide showed activity, albeit lower than that produced by cyclosporine. Intravenous immunoglobulins were effective both in parvovirus patients and in hypogammaglobulinemia cases. In salvage settings, alemtuzumab is active, particularly in large granular lymphocytic leukemia-associated cases. Other potentially useful salvage options include rituximab, anti-thymocyte globulin and bortezomib. The workup of acquired pure red cell aplasia should include investigations of common pathological associations. Most effective therapies are directed against T-cell-mediated immunity, and therapeutic choices need to account for associated conditions that may help in choosing alternative salvage agents, such as intravenous immunoglobulin, alemtuzumab and bortezomib.
Copyright© 2018 Ferrata Storti Foundation.
Figures
References
-
- Brown K, Young N. Parvovirus B19 infection and hematopoiesis. Blood Rev. 1995; 9(3):176–182. - PubMed
-
- Thompson DF, Gales MA. Drug-induced pure red cell aplasia. Pharmacotherapy. 1996;16(6):1002–1008. - PubMed
-
- Stohlman F, Quesenberry P, Howard D, Miller M, Schur P. Erythroid aplasia: an autoimmune complication of chronic lymphocytic leukemia. Clin Res. 1971;19:566.
-
- Masauzi N, Tanaka J, Watanabe M, et al. Primary Waldenström’s macroglobulinemia associated with pure red cell aplasia in which Ts/c lymphocytes inhibiting erythroid precursors were detected. [Rinsho ketsueki] Jpn J Clin Hematol. 1993; 34(3):355–361. - PubMed
-
- Kobayashi T, Hanada T, Sato Y, et al. A case of pure red cell aplasia with monoclonal gammopathy: immune-mediated inhibition of erythropoiesis. [Rinsho ketsueki] Jpn J Clin Hematol. 1987; 28(11): 2029–2033. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
