

Improvement of conformal arc plans by using deformable margin delineation method for stereotactic lung radiotherapy
- PMID: 29218841
- PMCID: PMC5768002
- DOI: 10.1002/acm2.12237
Improvement of conformal arc plans by using deformable margin delineation method for stereotactic lung radiotherapy
Abstract
Purpose: Stereotactic body radiotherapy (SBRT) is an established treatment technique in the management of medically inoperable early stage non-small cell lung cancer (NSCLC). Different techniques such as volumetric modulated arc (VMAT) and three-dimensional conformal arc (DCA) can be used in SBRT. Previously, it has been shown that VMAT is superior to DCA technique in terms of plan evaluation parameters. However, DCA technique has several advantages such as ease of use and considerable shortening of the treatment time. DCA technique usually results in worse conformity which is not possible to ameliorate by inverse optimization. In this study, we aimed to analyze whether a simple method - deformable margin delineation (DMD) - improves the quality of the DCA technique, reaching similar results to VMAT in terms of plan evaluation parameters.
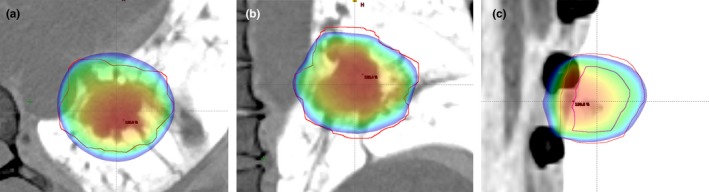
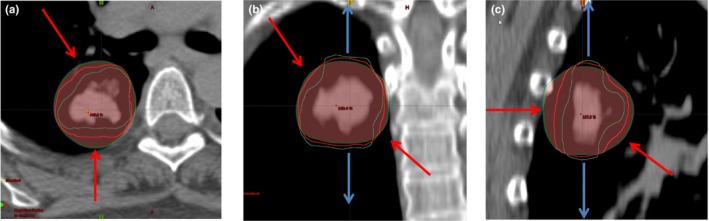
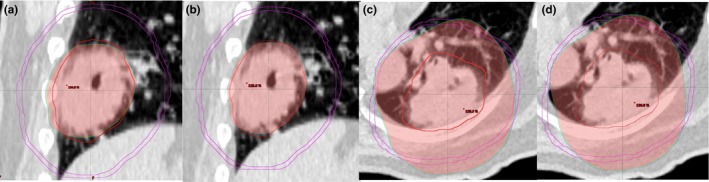
Methods: Twenty stage I-II (T1-2, N0, M0) NSCLC patients were included in this retrospective dosimetric study. Noncoplanar VMAT and conventional DCA plans were generated using 6 MV and 10 MV with flattening filter free (FFF) photon energies. The DCA plan with 6FFF was calculated and 95% of the PTV was covered by the prescription isodose line. Hot dose regions (receiving dose over 100% of prescription dose) outside PTV and cold dose regions (receiving dose under 100% of prescription dose) inside PTV were identified. A new PTV (PTV-DMD) was delineated by deforming PTV margin with respect to hot and cold spot regions obtained from conventional DCA plans. Dynamic multileaf collimators (MLC) were set to PTV-DMD beam eye view (BEV) positions and the new DCA plans (DCA-DMD) with 6FFF were generated. Three-dimensional (3D) dose calculations were computed for PTV-DMD volume. However, the prescription isodose was specified and normalized to cover 95% volume of original PTV. Several conformity indices and lung doses were compared for different treatment techniques.
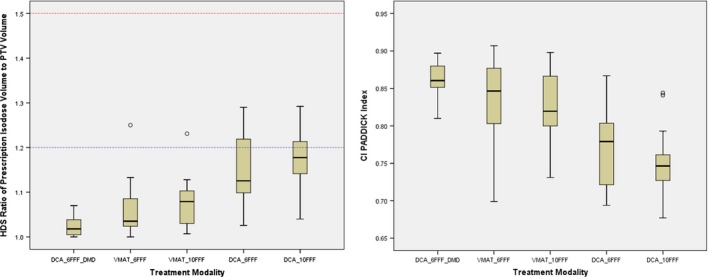
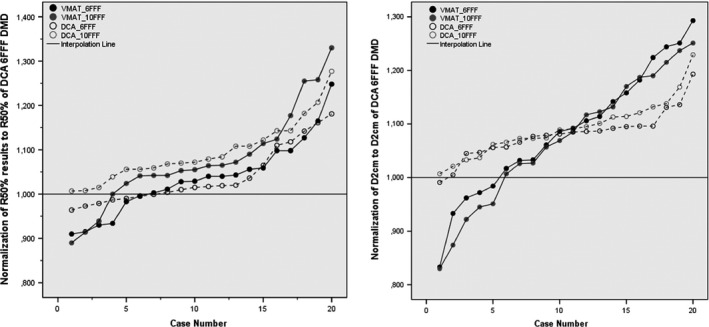
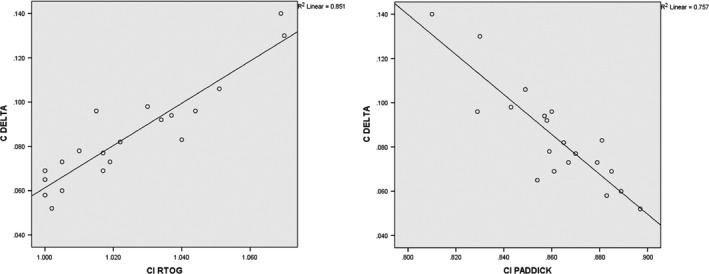
Results: DCA-DMD method significantly achieved a superior conformity index (CI), conformity number (CIPaddick ), gradient index (R50% ), isodose at 2 cm (D2 cm ) and external index (CΔ) with respect to VMAT and conventional DCA plans (P < 0.05 for all comparisons). CI ranged between 1.00-1.07 (Mean: 1.02); 1.00-1.18 (Mean: 1.06); 1.01-1.23 (Mean 1.08); 1.03-1.29 (Mean: 1.15); 1.04-1.29 (Mean: 1.18) for DCA-DMD-6FFF, VMAT-6FFF, VMAT-10FFF DCA-6FFF and DCA-10FFF respectively. DCA-DMD-6FFF technique resulted significantly better CI compared to others (P = 0.002; < 0.001; < 0.001; < 0.001). R50% ranged between 3.22-4.74 (Mean: 3.99); 3.24-5.92 (Mean: 4.15) for DCA-DMD-6FFF, VMAT-6FFF, respectively. DCA-DMD-6FFF technique resulted lower intermediate dose spillage compared to VMAT-6FFF, though the difference was statistically insignificant (P = 0.32). D2 cm ranged between 35.7% and 67.0% (Mean: 53.2%); 42.1%-79.2% (Mean: 57.8%) for DCA-DMD-6FFF, VMAT-6FFF respectively. DCA-DMD-6FFF have significantly better and sharp falloff gradient 2 cm away from PTV compared to VMAT-6FFF (P = 0.009). CΔ ranged between 0.052 and 0.140 (Mean: 0.085); 0,056-0,311 (Mean: 0.120) for DCA-DMD, VMAT-6FFF, respectively. DCA-DMD-6FFF have significantly improved CΔ (P = 0.002). VMAT- V20 Gy , V2.5 Gy and mean lung dose (MLD) indices are calculated to be 4.03%, 23.83%, 3.42 Gy and 4.19%, 27.88%,3.72 Gy, for DCA-DMD-6FFF and DCA techniques, respectively. DCA-DMD-6FFF achieved superior lung sparing compared to DCA technique. DCA-DMD-6FFF method reduced MUs 44% and 33% with respect to VMAT-6FFF and 10FFF, respectively, without sacrificing dose conformity (P < 0.001; P < 0.001).
Conclusions: Our results demonstrated that DCA plan evaluation parameters can be ameliorated by using the DMD method. This new method improves DCA plan quality and reaches similar results with VMAT in terms of dosimetric parameters. We believe that DCA-DMD is a simple and effective technique for SBRT and can be preferred due to shorter treatment and planning time.
Keywords: DCA; FFF; SBRT; VMAT.
© 2017 Acibadem University Department of Radiation Oncology. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Figures
References
-
- Lax I, Blomgren H, Naslund I, Svanstrom R. Stereotactic radiotherapy of malignancies in the abdomen. Methodological aspects. Acta Oncol. 33:677–683. - PubMed
-
- Uematsu M, Shioda A, Tahara K. Focal, high dose, and fractionated modified stereotactic radiation therapy for lung carcinoma patients: a preliminary experience. Cancer. 82:1062–1070. - PubMed
-
- Wulf J, Hadinger U, Oppitz U, et al. Stereotactic radiotherapy of extracranial targets: CT‐simulation and accuracy of treatment in the stereotactic body frame. Radiother Oncol. 57:225–236. - PubMed
-
- Herfarth KK, Debus J, Lohr F, et al. Extracranial stereotactic radiation therapy: set‐up accuracy of patients treated for liver metastases. Int J Radiat Oncol Biol Phys. 46:329–335. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
