

Intrathecal Morphine for Laparoscopic Segmental Colonic Resection as Part of an Enhanced Recovery Protocol: A Randomized Controlled Trial
- PMID: 29219935
- PMCID: PMC5794252
- DOI: 10.1097/AAP.0000000000000703
Intrathecal Morphine for Laparoscopic Segmental Colonic Resection as Part of an Enhanced Recovery Protocol: A Randomized Controlled Trial
Abstract
Background and objectives: Management of postoperative pain after laparoscopic segmental colonic resections remains controversial. We compared 2 methods of analgesia within an Enhanced Recovery After Surgery (ERAS) program. The goal of the study was to investigate whether administration of intrathecal bupivacaine/morphine would lead to an enhanced recovery.
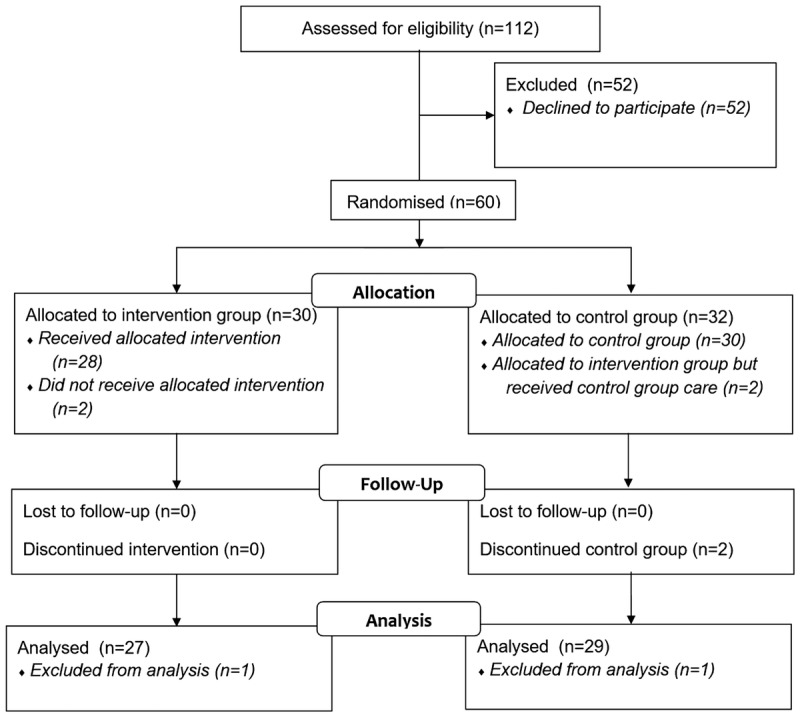
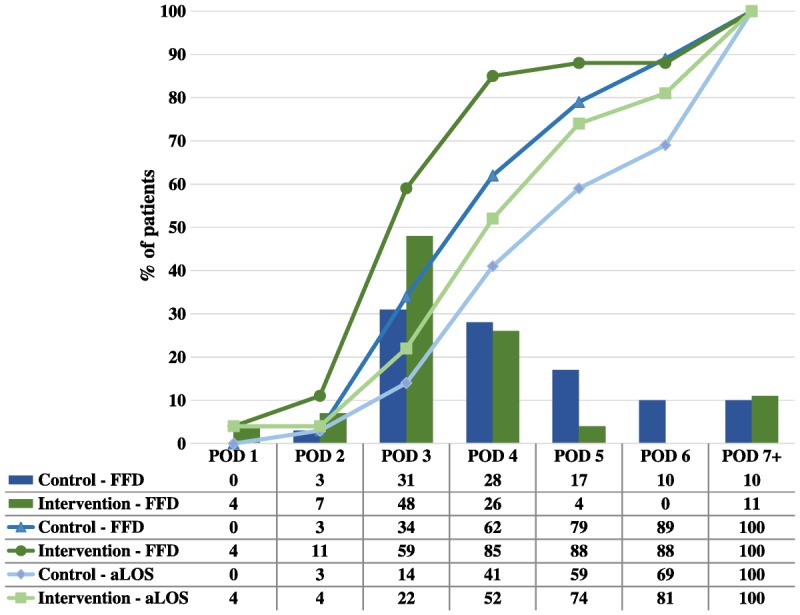
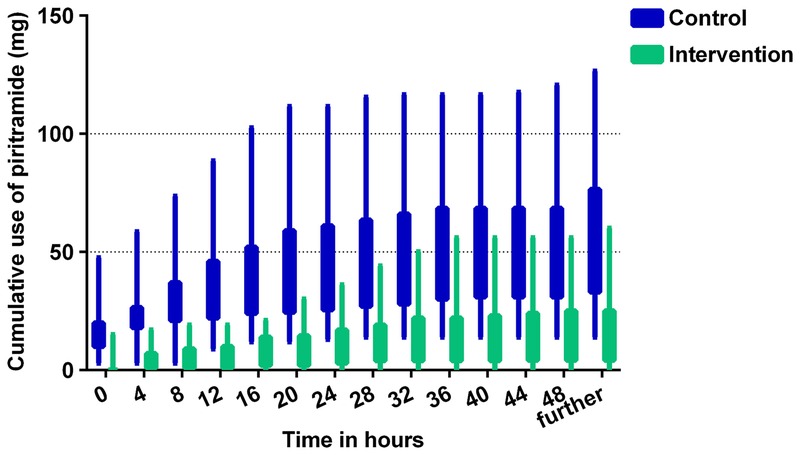
Methods: A single-center, randomized, double-blind controlled trial was performed (NL43488.101.13). Patients scheduled for laparoscopic segmental intestinal resections were considered. Exclusion criteria were patients in whom contraindications to spinal anesthesia were present, conversion to open surgery, and gastric and rectal surgery. The intervention group received single-shot intrathecal bupivacaine/morphine (12.5 mg/300 μg), with an altered dose for older patients. The control group received a sham procedure and a bolus of piritramide (0.1 mg/kg). Both groups received standardized general anesthesia and a patient-controlled intravenous analgesia pump as postoperative analgesia. All patients were treated according to an ERAS protocol. A decrease in days to "fit for discharge" was the primary outcome.
Results: Fifty-six patients were enrolled. Intervention group patients were fit for discharge earlier (median of 3 vs 4 days, P = 0.044). Furthermore, there was a significant decrease in opioid use and lower pain scores on the first postoperative day in the intervention group. There were no differences in adverse events (except for more pruritus), time to mobilization, fluid administration, or patient satisfaction.
Conclusions: This randomized controlled trial shows that intrathecal morphine is a more effective method of postoperative analgesia in laparoscopic surgery than intravenous opioids within an ERAS program. Recovery is faster and less painful with intrathecal morphine. Other studies have confirmed these results, although data on faster recovery are new and require confirmation in future trials.
Clinical trial registration: This study was registered at ClinicalTrials.gov, identifier NCT02284282.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gustafsson UO, Scott MJ, Schwenk W, et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS(®)) Society recommendations. World J Surg. 2013;37:259–284. - PubMed
-
- Levy BF, Scott MJ, Fawcett W, Fry C, Rockall TA. Randomized clinical trial of epidural, spinal or patient-controlled analgesia for patients undergoing laparoscopic colorectal surgery. Br J Surg. 2011;98:1068–1078. - PubMed
-
- Hubner M, Blanc C, Roulin D, Winiker M, Gander S, Demartines N. Randomized clinical trial on epidural versus patient-controlled analgesia for laparoscopic colorectal surgery within an enhanced recovery pathway. Ann Surg. 2015;261:648–653. - PubMed
-
- Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118:934–944. - PubMed
-
- Kong SK, Onsiong SM, Chiu WK, Li MK. Use of intrathecal morphine for postoperative pain relief after elective laparoscopic colorectal surgery. Anaesthesia. 2002;57:1168–1173. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical