

HIV prevention where it is needed most: comparison of strategies for the geographical allocation of interventions
- PMID: 29220115
- PMCID: PMC5810320
- DOI: 10.1002/jia2.25020
HIV prevention where it is needed most: comparison of strategies for the geographical allocation of interventions
Abstract
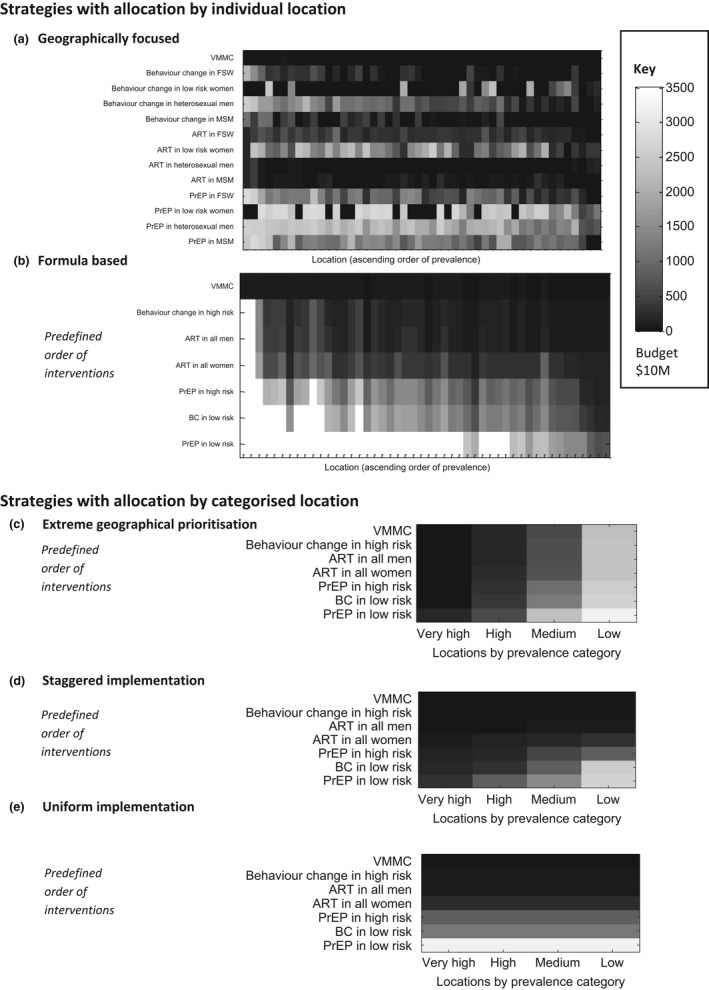
Introduction: A strategic approach to the application of HIV prevention interventions is a core component of the UNAIDS Fast Track strategy to end the HIV epidemic by 2030. Central to these plans is a focus on high-prevalence geographies, in a bid to target resources to those in greatest need and maximize the reduction in new infections. Whilst this idea of geographical prioritization has the potential to improve efficiency, it is unclear how it should be implemented in practice. There are a range of prevention interventions which can be applied differentially across risk groups and locations, making allocation decisions complex. Here, we use mathematical modelling to compare the impact (infections averted) of a number of different approaches to the implementation of geographical prioritization of prevention interventions, similar to those emerging in policy and practice, across a range of prevention budgets.
Methods: We use geographically specific mathematical models of the epidemic and response in 48 counties and major cities of Kenya to project the impact of the different geographical prioritization approaches. We compare the geographical allocation strategies with a nationally uniform approach under which the same interventions must be applied across all modelled locations.
Results: We find that the most extreme geographical prioritization strategy, which focuses resources exclusively to high-prevalence locations, may substantially restrict impact (41% fewer infections averted) compared to a nationally uniform approach, as opportunities for highly effective interventions for high-risk populations in lower-prevalence areas are missed. Other geographical allocation approaches, which intensify efforts in higher-prevalence areas whilst maintaining a minimum package of cost-effective interventions everywhere, consistently improve impact at all budget levels. Such strategies balance the need for greater investment in locations with the largest epidemics whilst ensuring higher-risk groups in lower-priority locations are provided with cost-effective interventions.
Conclusions: Our findings serve as a warning to not be too selective in the application of prevention strategies. Further research is needed to understand how decision-makers can find the right balance between the choice of interventions, focus on high-risk populations, and geographical targeting to ensure the greatest impact of HIV prevention.
Keywords: HIV prevention; epidemiology; geographical prioritization; health policy; mathematical modelling; resource allocation.
© 2017 The Authors. Journal of the International AIDS Society published by John Wiley & sons Ltd on behalf of the International AIDS Society.
Figures

References
-
- Anderson SJ, Cherutich P, Kilonzo N, Cremin I, Fecht D, Kimanga D, et al. Maximising the effect of combination HIV prevention through prioritisation of the people and places in greatest need: a modelling study. Lancet. 2014;384(9939):249–56. - PubMed
-
- Tanser F, LeSueur D, Solarsh G, Wilkinson D. HIV heterogeneity and proximity of homestead to roads in rural South Africa: an exploration using a geographical information system. Trop Med Int Health. 2000;5(1):40–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
