

Effects of Rate on Analgesia in Kilohertz Frequency Spinal Cord Stimulation: Results of the PROCO Randomized Controlled Trial
- PMID: 29220121
- PMCID: PMC5814855
- DOI: 10.1111/ner.12746
Effects of Rate on Analgesia in Kilohertz Frequency Spinal Cord Stimulation: Results of the PROCO Randomized Controlled Trial
Abstract
Objective: The PROCO RCT is a multicenter, double-blind, crossover, randomized controlled trial (RCT) that investigated the effects of rate on analgesia in kilohertz frequency (1-10 kHz) spinal cord stimulation (SCS).
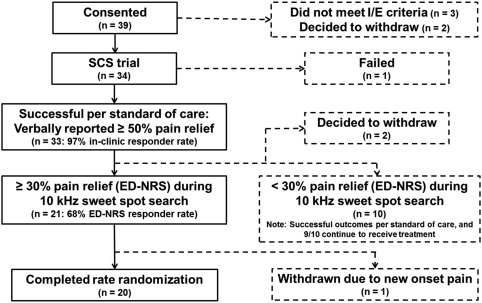
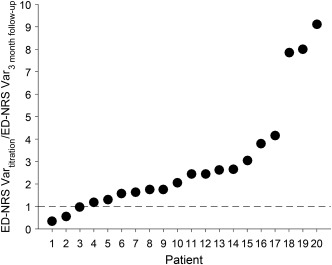
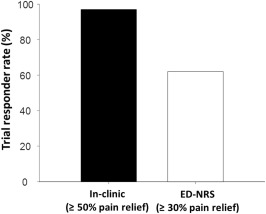
Materials and methods: Patients were implanted with SCS systems and underwent an eight-week search to identify the best location ("sweet spot") of stimulation at 10 kHz within the searched region (T8-T11). An electronic diary (e-diary) prompted patients for pain scores three times per day. Patients who responded to 10 kHz per e-diary numeric rating scale (ED-NRS) pain scores proceeded to double-blind rate randomization. Patients received 1, 4, 7, and 10 kHz SCS at the same sweet spot found for 10 kHz in randomized order (four weeks at each frequency). For each frequency, pulse width and amplitude were titrated to optimize therapy.
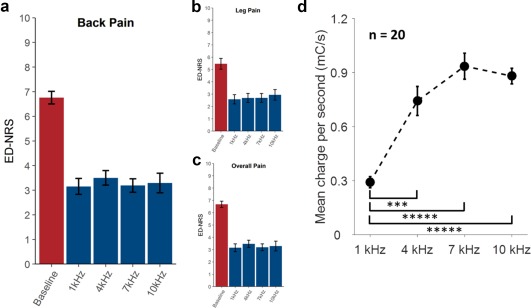
Results: All frequencies provided equivalent pain relief as measured by ED-NRS (p ≤ 0.002). However, mean charge per second differed across frequencies, with 1 kHz SCS requiring 60-70% less charge than higher frequencies (p ≤ 0.0002).
Conclusions: The PROCO RCT provides Level I evidence for equivalent pain relief from 1 to 10 kHz with appropriate titration of pulse width and amplitude. 1 kHz required significantly less charge than higher frequencies.
Keywords: Chronic pain; PROCO; double-blind; high frequency; high frequency SCS; kilohertz SCS; randomized controlled trial; sub-perception SCS.
© 2017 The Authors. Neuromodulation: Technology at the Neural Interface published by Wiley Periodicals, Inc. on behalf of International Neuromodulation Society.
Figures

Similar articles
-
Clinical Outcomes of 1 kHz Subperception Spinal Cord Stimulation in Implanted Patients With Failed Paresthesia-Based Stimulation: Results of a Prospective Randomized Controlled Trial.Neuromodulation. 2016 Oct;19(7):731-737. doi: 10.1111/ner.12441. Epub 2016 May 17. Neuromodulation. 2016. PMID: 27186822 Clinical Trial.
-
Long-term quality of life improvement for chronic intractable back and leg pain patients using spinal cord stimulation: 12-month results from the SENZA-RCT.Qual Life Res. 2018 Aug;27(8):2035-2044. doi: 10.1007/s11136-018-1890-8. Epub 2018 Jun 1. Qual Life Res. 2018. PMID: 29858746 Clinical Trial.
-
Efficacy of different spinal cord stimulation paradigms for the treatment of chronic neuropathic pain (PARS-trial): study protocol for a double-blinded, randomized, and placebo-controlled crossover trial.Trials. 2021 Jan 25;22(1):87. doi: 10.1186/s13063-020-05013-7. Trials. 2021. PMID: 33494781 Free PMC article.
-
Pain relief and improvement in quality of life with 10 kHz SCS therapy: Summary of clinical evidence.CNS Neurosci Ther. 2020 Apr;26(4):403-415. doi: 10.1111/cns.13285. Epub 2020 Feb 22. CNS Neurosci Ther. 2020. PMID: 32087613 Free PMC article. Review.
-
10-kHz High-Frequency Spinal Cord Stimulation for Adults With Chronic Noncancer Pain: A Health Technology Assessment.Ont Health Technol Assess Ser. 2020 Mar 6;20(6):1-109. eCollection 2020. Ont Health Technol Assess Ser. 2020. PMID: 32194881 Free PMC article.
Cited by
-
Spinal Cord Stimulation for Painful Diabetic Neuropathy.J Diabetes Sci Technol. 2024 Jan;18(1):168-192. doi: 10.1177/19322968221133795. Epub 2022 Nov 17. J Diabetes Sci Technol. 2024. PMID: 36384312 Free PMC article. Review.
-
Glia to neuron ratio in the posterior aspect of the human spinal cord at thoracic segments relevant to spinal cord stimulation.J Anat. 2019 Nov;235(5):997-1006. doi: 10.1111/joa.13061. Epub 2019 Jul 26. J Anat. 2019. PMID: 31347695 Free PMC article.
-
The Evolution of Neuromodulation in the Treatment of Chronic Pain: Forward-Looking Perspectives.Pain Med. 2019 Jun 1;20(Suppl 1):S58-S68. doi: 10.1093/pm/pnz074. Pain Med. 2019. PMID: 31152176 Free PMC article. Review.
-
Research design considerations for randomized controlled trials of spinal cord stimulation for pain: Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials/Institute of Neuromodulation/International Neuromodulation Society recommendations.Pain. 2021 Jul 1;162(7):1935-1956. doi: 10.1097/j.pain.0000000000002204. Pain. 2021. PMID: 33470748 Free PMC article.
-
Temporary trigeminal ganglion stimulation can improve zoster-related trigeminal neuralgia: a retrospective study in a single center.Front Neurol. 2025 Jan 7;15:1513867. doi: 10.3389/fneur.2024.1513867. eCollection 2024. Front Neurol. 2025. PMID: 39839867 Free PMC article.
References
-
- Kapural L, Yu C, Doust MW et al. Novel 10‐kHz high‐frequency therapy (HF10 Therapy) is superior to traditional low‐frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA‐RCT randomized controlled trial. Anesthesiology 2015;123:851–860. - PubMed
-
- Deer T, Slavin KV, Amirdelfan K et al. Success using neuromodulation with BURST (SUNBURST) study: results from a prospective, randomized controlled trial using a novel burst waveform. Neuromodulation 2018;21:56–66. - PubMed
-
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965;150:970–979. - PubMed
-
- Lempka SF, McIntyre CC, Kilgore KL et al. Computational analysis of kilohertz frequency spinal cord stimulation for chronic pain management. Anesthesiology 2015;122:1362–1376. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
