

Interpreting ambiguous 'trace' results in Schistosoma mansoni CCA Tests: Estimating sensitivity and specificity of ambiguous results with no gold standard
- PMID: 29220354
- PMCID: PMC5738141
- DOI: 10.1371/journal.pntd.0006102
Interpreting ambiguous 'trace' results in Schistosoma mansoni CCA Tests: Estimating sensitivity and specificity of ambiguous results with no gold standard
Abstract
Background: The development of new diagnostics is an important tool in the fight against disease. Latent Class Analysis (LCA) is used to estimate the sensitivity and specificity of tests in the absence of a gold standard. The main field diagnostic for Schistosoma mansoni infection, Kato-Katz (KK), is not very sensitive at low infection intensities. A point-of-care circulating cathodic antigen (CCA) test has been shown to be more sensitive than KK. However, CCA can return an ambiguous 'trace' result between 'positive' and 'negative', and much debate has focused on interpretation of traces results.
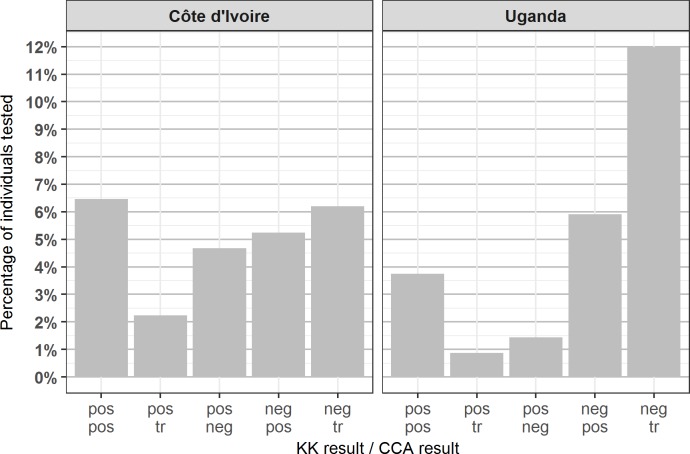
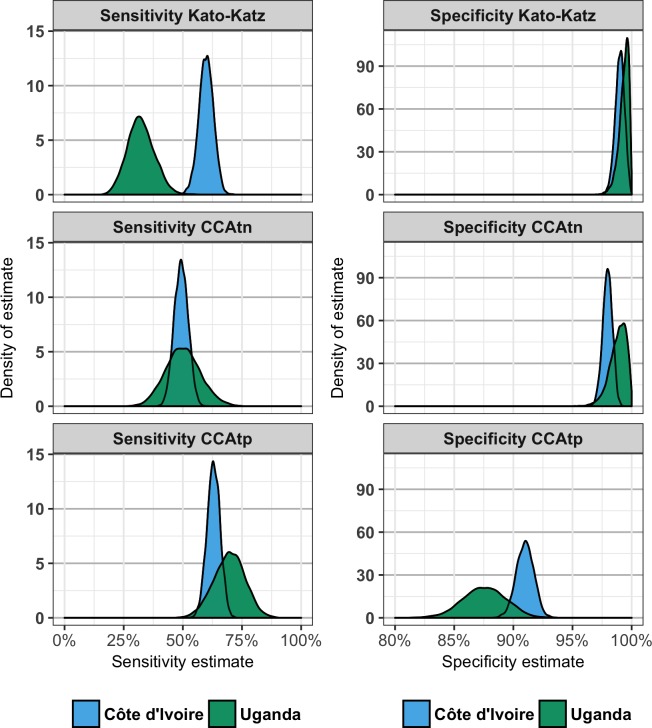
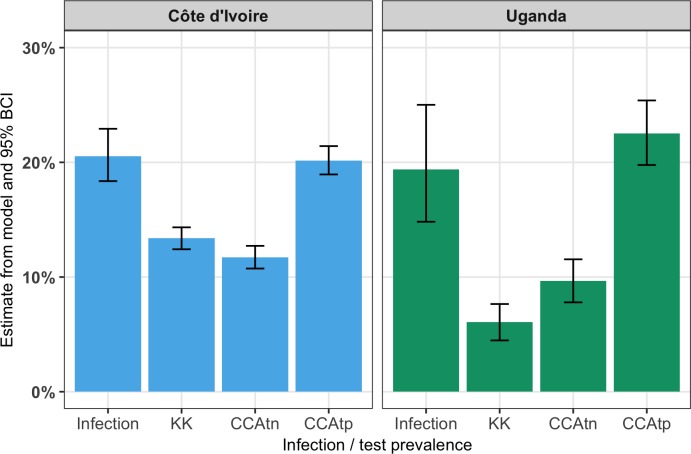
Methodology/principle findings: We show how LCA can be extended to include ambiguous trace results and analyse S. mansoni studies from both Côte d'Ivoire (CdI) and Uganda. We compare the diagnostic performance of KK and CCA and the observed results by each test to the estimated infection prevalence in the population. Prevalence by KK was higher in CdI (13.4%) than in Uganda (6.1%), but prevalence by CCA was similar between countries, both when trace was assumed to be negative (CCAtn: 11.7% in CdI and 9.7% in Uganda) and positive (CCAtp: 20.1% in CdI and 22.5% in Uganda). The estimated sensitivity of CCA was more consistent between countries than the estimated sensitivity of KK, and estimated infection prevalence did not significantly differ between CdI (20.5%) and Uganda (19.1%). The prevalence by CCA with trace as positive did not differ significantly from estimates of infection prevalence in either country, whereas both KK and CCA with trace as negative significantly underestimated infection prevalence in both countries.
Conclusions: Incorporation of ambiguous results into an LCA enables the effect of different treatment thresholds to be directly assessed and is applicable in many fields. Our results showed that CCA with trace as positive most accurately estimated infection prevalence.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Sustaining the drive to overcome the global impact of neglected tropical diseases: second WHO report on neglected tropical diseases: summary. 2013.
-
- Lai Y-S, Biedermann P, Ekpo UF, Garba A, Mathieu E, Midzi N, et al. Spatial distribution of schistosomiasis and treatment needs in sub-Saharan Africa: a systematic review and geostatistical analysis. The Lancet Infectious Diseases. 2015;15(8):927–40. doi: 10.1016/S1473-3099(15)00066-3 - DOI - PubMed
-
- Lo NC, Addiss DG, Hotez PJ, King CH, Stothard JR, Evans DS, et al. A call to strengthen the global strategy against schistosomiasis and soil-transmitted helminthiasis: the time is now. The Lancet Infectious Diseases. 2017;17(2):e64–e9. doi: 10.1016/S1473-3099(16)30535-7 - DOI - PMC - PubMed
-
- King CH. It's Time to Dispel the Myth of "Asymptomatic" Schistosomiasis. PLoS Negl Trop Dis. 2015;9(2):e0003504 doi: 10.1371/journal.pntd.0003504 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
