

Can mother-to-child transmission of HIV be eliminated without addressing the issue of stigma? Modeling the case for a setting in South Africa
- PMID: 29220369
- PMCID: PMC5722282
- DOI: 10.1371/journal.pone.0189079
Can mother-to-child transmission of HIV be eliminated without addressing the issue of stigma? Modeling the case for a setting in South Africa
Abstract
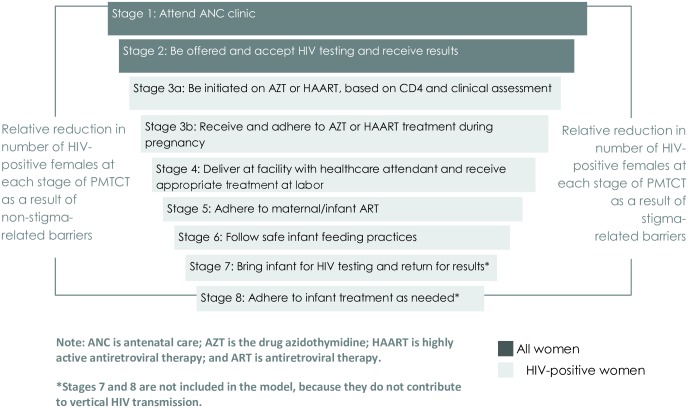
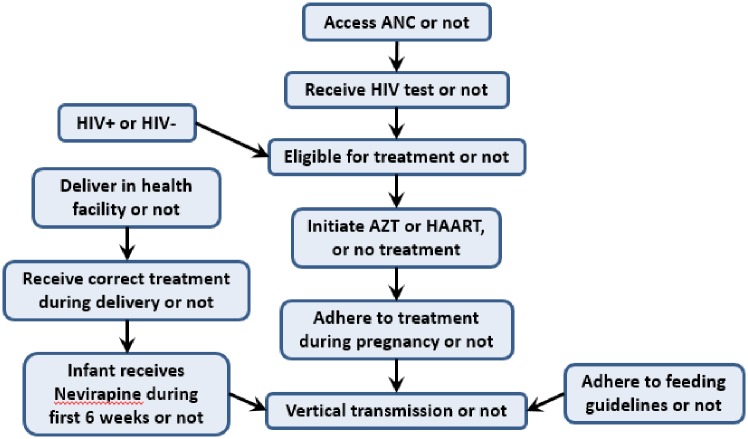
Background: Stigma and discrimination ontinue to undermine the effectiveness of the HIV response. Despite a growing body of evidence of the negative relationship between stigma and HIV outcomes, there is a paucity of data available on the prevalence of stigma and its impact. We present a probabilistic cascade model to estimate the magnitude of impact stigma has on mother-to-child-transmission (MTCT).
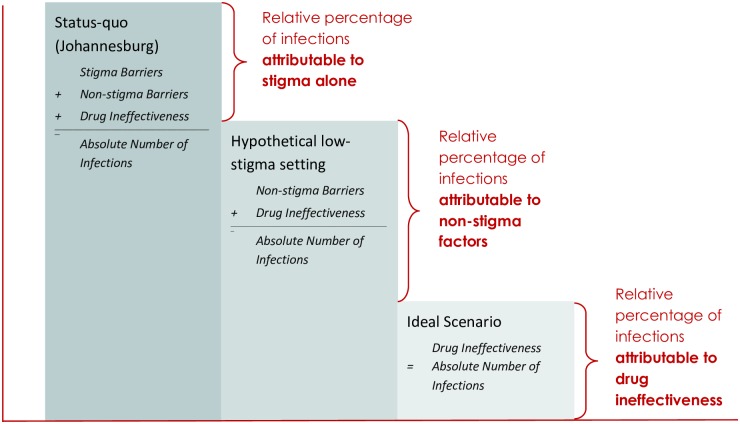
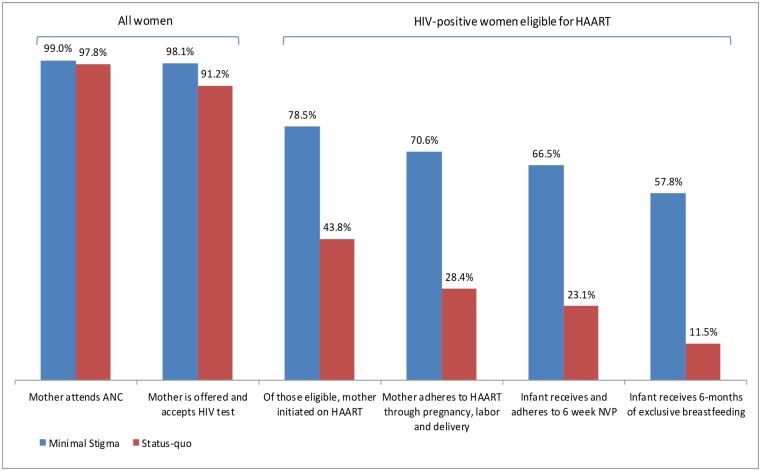
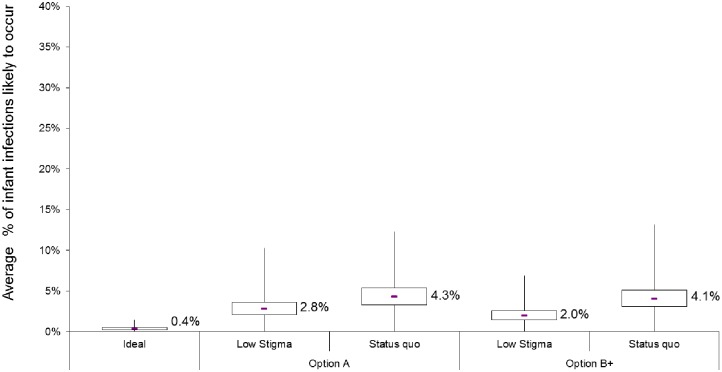
Methods: The model was parameterized using 2010 data from Johannesburg, South Africa, from which loss-to-care at each stage of the antenatal cascade were available. Three scenarios were compared to assess the individual contributions of stigma, non-stigma related barriers, and drug ineffectiveness on the overall number of infant infections. Uncertainty analysis was used to estimate plausible ranges. The model follows the guidelines in place in 2010 when the data were extracted (WHO Option A), and compares this with model results had Option B+ been implemented at the time.
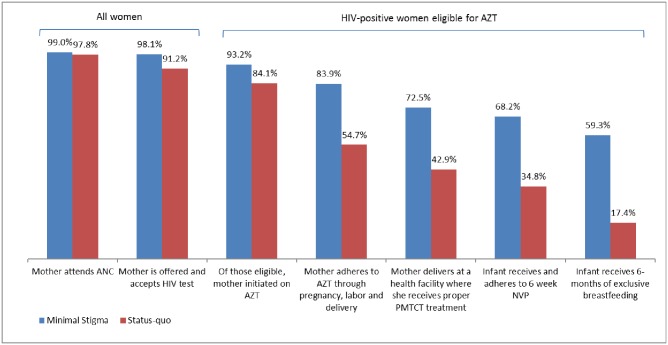
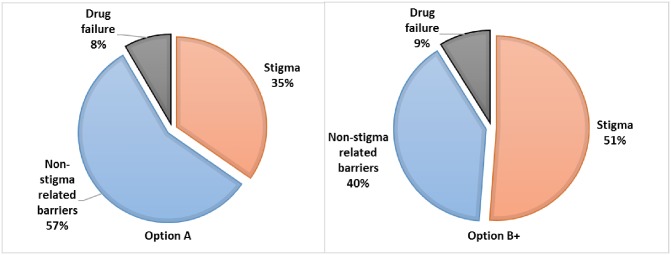
Results: The model estimated under Option A, 35% of infant infections being attributed to stigma. This compares to 51% of total infections had Option B+ been implemented in 2010. Under Option B+, the model estimated fewer infections than Option A, due to the availability of more effective drugs. Only 8% (Option A) and 9% (Option B+) of infant infections were attributed to drug ineffectiveness, with the trade-off in the proportion of infections being between stigma and non-stigma-related barriers.
Conclusions: The model demonstrates that while the effect of stigma on retention of women at any given stage along the cascade can be relatively small, the cumulative effect can be large. Reducing stigma may be critical in reaching MTCT elimination targets, because as countries improve supply-side factors, the relative impact of stigma becomes greater. The cumulative nature of the PMTCT cascade results in stigma having a large effect, this feature may be harnessed for efficiency in investment by prioritizing interventions that can affect multiple stages of the cascade simultaneously.
Conflict of interest statement
Figures
Similar articles
-
Understanding women's uptake and adherence in Option B+ for prevention of mother-to-child HIV transmission in Papua, Indonesia: A qualitative study.PLoS One. 2018 Jun 18;13(6):e0198329. doi: 10.1371/journal.pone.0198329. eCollection 2018. PLoS One. 2018. PMID: 29912960 Free PMC article.
-
Effect of a multicomponent behavioural PMTCT cluster randomised controlled trial on HIV stigma reduction among perinatal HIV positive women in Mpumalanga province, South Africa.SAHARA J. 2018 Dec;15(1):80-88. doi: 10.1080/17290376.2018.1510787. SAHARA J. 2018. PMID: 30134772 Free PMC article. Clinical Trial.
-
Option B+ Program for the Prevention of Vertical Transmission of HIV: A Case Study in Johannesburg, South Africa.Front Public Health. 2020 Oct 28;8:533534. doi: 10.3389/fpubh.2020.533534. eCollection 2020. Front Public Health. 2020. PMID: 33194942 Free PMC article.
-
Uptake of guidelines on prevention of mother-to-child transmission of HIV in rural Tanzania: time for change.Swiss Med Wkly. 2013 Mar 14;143:w13775. doi: 10.4414/smw.2013.13775. eCollection 2013. Swiss Med Wkly. 2013. PMID: 23519621 Review.
-
Medication adherence in pregnant women with human immunodeficiency virus receiving antiretroviral therapy in sub-Saharan Africa: a systematic review.BMC Public Health. 2018 Jun 27;18(1):805. doi: 10.1186/s12889-018-5651-y. BMC Public Health. 2018. PMID: 29945601 Free PMC article.
Cited by
-
A universal precautions approach to reducing stigma in health care: getting beyond HIV-specific stigma.Harm Reduct J. 2022 Jul 7;19(1):74. doi: 10.1186/s12954-022-00658-w. Harm Reduct J. 2022. PMID: 35799296 Free PMC article. Review.
-
Stigma toward people living with HIV among healthcare providers in midwifery hospitals in Shenzhen, China from 2020 to 2023.Sci Rep. 2025 Feb 24;15(1):6677. doi: 10.1038/s41598-025-91263-x. Sci Rep. 2025. PMID: 39994321 Free PMC article.
-
Client Experiences in a Mobile-Phone Counseling Intervention for Enhancing Access to Prevention of Mother To-Child Transmission (PMTCT) Services in Kenya.Front Glob Womens Health. 2022 Jun 3;3:785194. doi: 10.3389/fgwh.2022.785194. eCollection 2022. Front Glob Womens Health. 2022. PMID: 35720809 Free PMC article.
-
HIV/AIDS-related stigma and discrimination among healthcare providers in Western China: a population-based cross-sectional study.BMC Infect Dis. 2025 Jul 28;25(1):951. doi: 10.1186/s12879-025-11311-9. BMC Infect Dis. 2025. PMID: 40722071 Free PMC article.
-
Maternal and infant antiretroviral therapy adherence among women living with HIV in rural South Africa: a cluster randomised trial of the role of male partner participation on adherence and PMTCT uptake.SAHARA J. 2021 Dec;18(1):17-25. doi: 10.1080/17290376.2020.1863854. SAHARA J. 2021. PMID: 33641621 Free PMC article. Clinical Trial.
References
-
- UNAIDS. 90-90-90 An ambitious treatment target to help end the AIDS epidemic. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS, 2014.
-
- UNAIDS. Count Down to Zero: Global play towards the elimination of new HIV infections among children by 2015 and keeping their mothers alive Geneva, Switzerland: UNAIDS, 2011.
-
- U.S. Department of State. Pepfar 3.0 Controlling the Epidemic: Delivering on the Promise of an AIDS-free Generation. Washington, DC: The Office of the U.S. Global AIDS Coordinator, 2014.
-
- UNICEF. UNICEF’s HIV/AIDS Programme Vision and Direction for Action 2014–2017. UNICEF, 2013.
-
- Piot P, Karim SSA, Hecht R, Legido-Quigley H, Buse K, Stover J, et al. A UNAIDS–Lancet Commission on Defeating AIDS—Advancing Global Health Defeating AIDS—advancing global health. Lancet. 2015;386:171–218. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
