

Prediction of Radiation Esophagitis in Non-Small Cell Lung Cancer Using Clinical Factors, Dosimetric Parameters, and Pretreatment Cytokine Levels
- PMID: 29220828
- PMCID: PMC6002355
- DOI: 10.1016/j.tranon.2017.11.005
Prediction of Radiation Esophagitis in Non-Small Cell Lung Cancer Using Clinical Factors, Dosimetric Parameters, and Pretreatment Cytokine Levels
Abstract
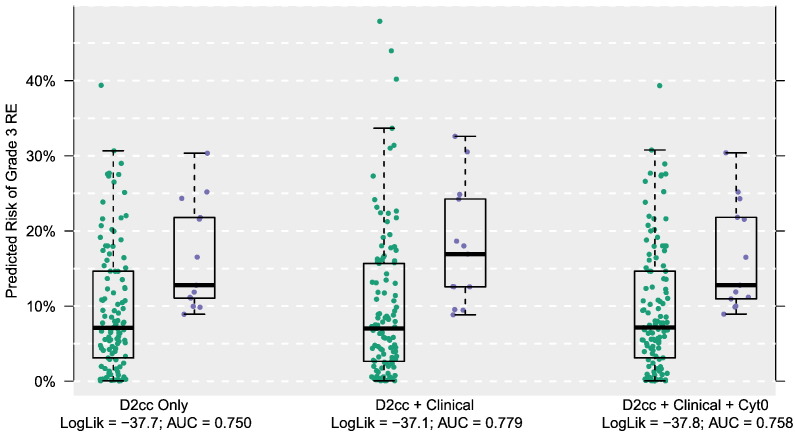
Radiation esophagitis (RE) is a common adverse event associated with radiotherapy for non-small cell lung cancer (NSCLC). While plasma cytokine levels have been correlated with other forms of radiation-induced toxicity, their association with RE has been less well studied. We analyzed data from 126 patients treated on 4 prospective clinical trials. Logistic regression models based on combinations of dosimetric factors [maximum dose to 2 cubic cm (D2cc) and generalized equivalent uniform dose (gEUD)], clinical variables, and pretreatment plasma levels of 30 cytokines were developed. Cross-validated estimates of area under the receiver operating characteristic curve (AUC) and log likelihood were used to assess prediction accuracy. Dose-only models predicted grade 3 RE with AUC values of 0.750 (D2cc) and 0.727 (gEUD). Combining clinical factors with D2cc increased the AUC to 0.779. Incorporating pretreatment cytokine measurements, modeled as direct associations with RE and as potential interactions with the dose-esophagitis association, produced AUC values of 0.758 and 0.773, respectively. D2cc and gEUD correlated with grade 3 RE with odds ratios (ORs) of 1.094/Gy and 1.096/Gy, respectively. Female gender was associated with a higher risk of RE, with ORs of 1.09 and 1.112 in the D2cc and gEUD models, respectively. Older age was associated with decreased risk of RE, with ORs of 0.992/year and 0.991/year in the D2cc and gEUD models, respectively. Combining clinical with dosimetric factors but not pretreatment cytokine levels yielded improved prediction of grade 3 RE compared to prediction by dose alone. Such multifactorial modeling may prove useful in directing radiation treatment planning.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Dosimetric predictors for acute esophagitis during radiation therapy for lung cancer: Results of a large statewide observational study.Pract Radiat Oncol. 2018 May-Jun;8(3):167-173. doi: 10.1016/j.prro.2017.07.010. Epub 2017 Jul 19. Pract Radiat Oncol. 2018. PMID: 28919249 Free PMC article.
-
Radiation-induced lung toxicity in non-small-cell lung cancer: Understanding the interactions of clinical factors and cytokines with the dose-toxicity relationship.Radiother Oncol. 2017 Oct;125(1):66-72. doi: 10.1016/j.radonc.2017.09.005. Epub 2017 Sep 23. Radiother Oncol. 2017. PMID: 28947099 Free PMC article.
-
A model combining age, equivalent uniform dose and IL-8 may predict radiation esophagitis in patients with non-small cell lung cancer.Radiother Oncol. 2018 Mar;126(3):506-510. doi: 10.1016/j.radonc.2017.12.026. Radiother Oncol. 2018. PMID: 29496281 Free PMC article.
-
Enhanced prediction of postoperative radiotherapy-induced esophagitis in non-small cell lung cancer: Dosiomic model development in a real-world cohort and validation in the PORT-C randomized controlled trial.Thorac Cancer. 2023 Oct;14(28):2839-2845. doi: 10.1111/1759-7714.15068. Epub 2023 Aug 19. Thorac Cancer. 2023. PMID: 37596813 Free PMC article. Clinical Trial.
-
Clinical and dosimetric predictors of radiation-induced esophageal toxicity.Int J Radiat Oncol Biol Phys. 1999 Aug 1;45(1):97-103. doi: 10.1016/s0360-3016(99)00163-7. Int J Radiat Oncol Biol Phys. 1999. PMID: 10477012
Cited by
-
Research progress of radiation esophagitis: A narrative review.Medicine (Baltimore). 2025 May 9;104(19):e42273. doi: 10.1097/MD.0000000000042273. Medicine (Baltimore). 2025. PMID: 40355243 Free PMC article. Review.
-
Significance of radiation esophagitis: Conditional survival assessment in patients with non-small cell lung cancer.J Natl Cancer Cent. 2021 Feb 18;1(2):31-38. doi: 10.1016/j.jncc.2021.02.003. eCollection 2021 Jun. J Natl Cancer Cent. 2021. PMID: 39035770 Free PMC article.
-
Dosimetric risk factors for radiation esophagitis in patients with breast cancer following regional nodal radiation.World J Clin Cases. 2024 Jun 16;12(17):2995-3003. doi: 10.12998/wjcc.v12.i17.2995. World J Clin Cases. 2024. PMID: 38898857 Free PMC article.
-
Machine learning highlights the deficiency of conventional dosimetric constraints for prevention of high-grade radiation esophagitis in non-small cell lung cancer treated with chemoradiation.Clin Transl Radiat Oncol. 2020 Mar 24;22:69-75. doi: 10.1016/j.ctro.2020.03.007. eCollection 2020 May. Clin Transl Radiat Oncol. 2020. PMID: 32274426 Free PMC article.
-
Multi-omics to predict acute radiation esophagitis in patients with lung cancer treated with intensity-modulated radiation therapy.Eur J Med Res. 2023 Mar 19;28(1):126. doi: 10.1186/s40001-023-01041-6. Eur J Med Res. 2023. PMID: 36935504 Free PMC article.
References
-
- Auperin A, Le Pechoux C, Rolland E. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non–small-cell lung cancer. J Clin Oncol. 2010;28:2181–2190. - PubMed
-
- Werner-Wasik M, Paulus R, Curran WJ., Jr. Acute esophagitis and late lung toxicity in concurrent chemoradiotherapy trials in patients with locally advanced non–small-cell lung cancer: analysis of the Radiation Therapy Oncology Group (RTOG) database. Clin Lung Cancer. 2011;12:245–251. - PubMed
-
- Trotti A, Colevas AD, Setser A. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol. 2003;13:176–181. - PubMed
-
- Cox JD, Pajak TF, Asbell S. Interruptions of high-dose radiation therapy decrease long-term survival of favorable patients with unresectable non–small cell carcinoma of the lung: analysis of 1244 cases from 3 Radiation Therapy Oncology Group (RTOG) trials. Int J Radiat Oncol Biol Phys. 1993;27:493–498. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
