

Goal-directed fluid restriction using stroke volume variation and cardiac index during one-lung ventilation: a randomized controlled trial
- PMID: 29221272
- PMCID: PMC5708410
- DOI: 10.21037/jtd.2017.08.98
Goal-directed fluid restriction using stroke volume variation and cardiac index during one-lung ventilation: a randomized controlled trial
Abstract
Background: Goal-directed therapy confers a strong prognosis in patients undergoing major cardiac or noncardiac surgery. The present study investigated whether intraoperative goal-directed fluid restriction (GDFR) using stroke volume variation (SVV) and cardiac index could improve oxygenation and postoperative outcome in patients undergoing one-lung ventilation (OLV).
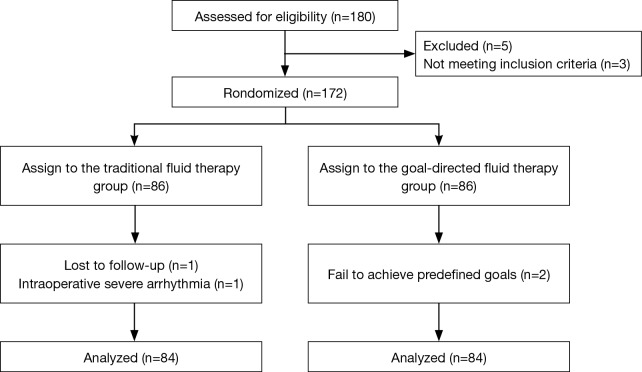
Methods: A Total of 168 patients scheduled for elective thoracoscopic lobectomy under OLV were randomized into the GDFR protocol (group G) or conventional fluid therapy groups (group C). Patients in group C underwent conventional fluid therapy based on mean arterial pressure (MAP), central venous pressure (CVP), and urine volume, whereas those in group G received GDFR protocol associated with the SVV from 10-13% and the cardiac index was controlled at a minimum of 2.5 L/min/m2. The primary outcome variable was PaO2/FiO2. The secondary outcomes were other pulmonary variables and lung mechanics, inflammatory response, the incidence of postoperative pulmonary complications, and the length of hospital stay.
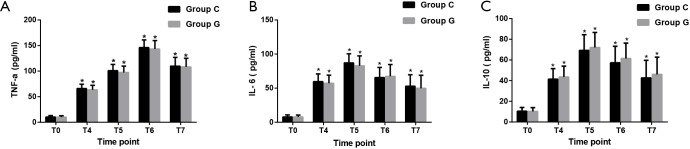
Results: During surgery, the PaO2/FiO2 ratio in group G was more than that of group C at 30 and 60 min after OLV, 10 min after re-expansion, and the end of the operation (259±29 vs. 314±34; 253±30 vs. 308±35; 341±34 vs. 394±39; 349±35 vs. 401±39, respectively, all P<0.001). Compared to conventional fluid therapy, GDFR protocol also significantly improved the hemodynamic and lung mechanics with the initiation of OLV. The incidence of postoperative pulmonary complications such as acute lung injury and pneumonia, and the length of hospital stay were decreased by GDFR protocol as compared to conventional fluid therapy (all P<0.05). However, there were no significant differences between groups with respect to the concentration of serum tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-10 (IL-10).
Conclusions: The GDFR protocol based on SVV and cardiac index applied in patients undergoing OLV improves intraoperative pulmonary oxygenation. It can also reduce the postoperative complications and length of hospital stay. However, the GDFR strategy cannot reduce the local or systemic inflammation.
Trial registration: Chinese Clinical Trials Register ChiCTR-INR-16008288, Registered 20 April, 2016.
Keywords: Fluid therapy; lung function; one-lung ventilation (OLV); stroke volume variation (SVV).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures



References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous