

Living-related lung transplantation
- PMID: 29221321
- PMCID: PMC5708411
- DOI: 10.21037/jtd.2017.08.152
Living-related lung transplantation
Abstract
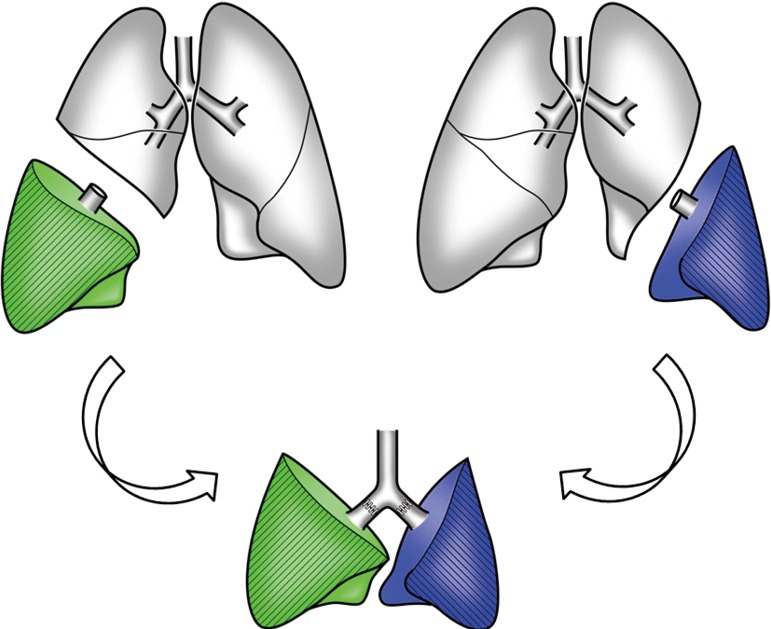
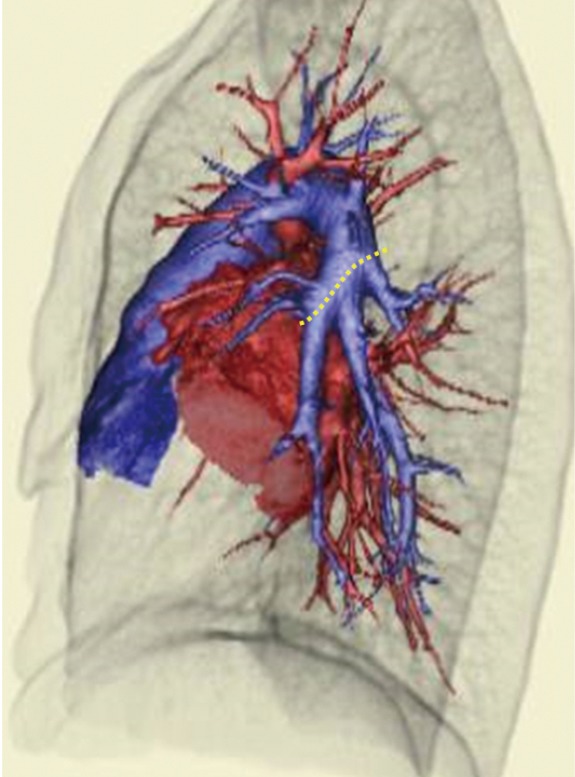
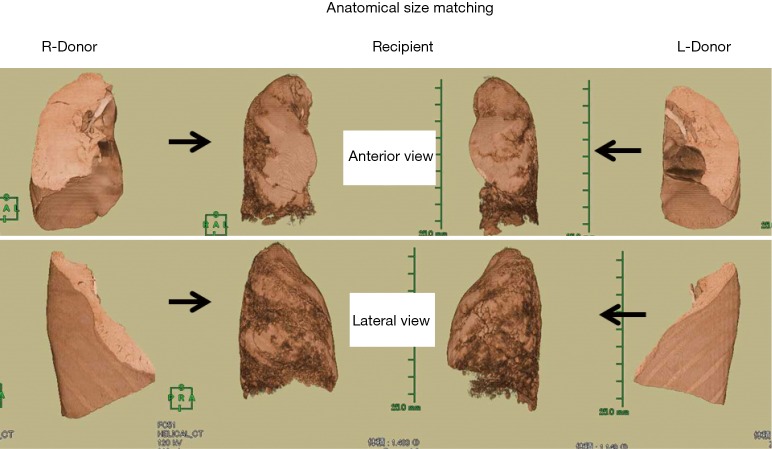
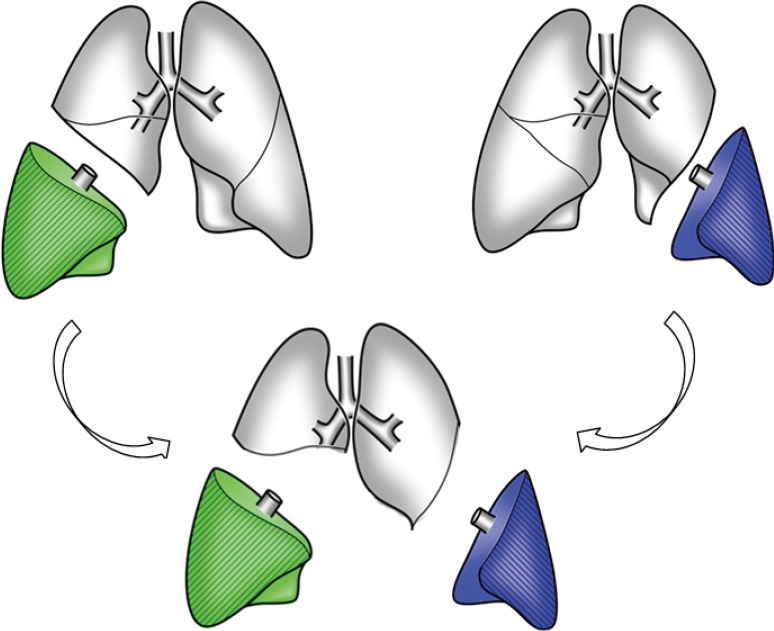
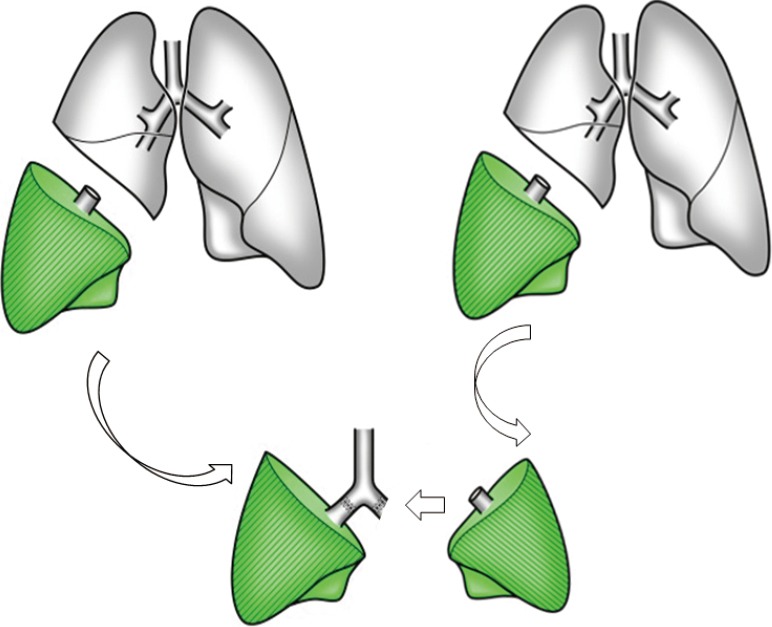
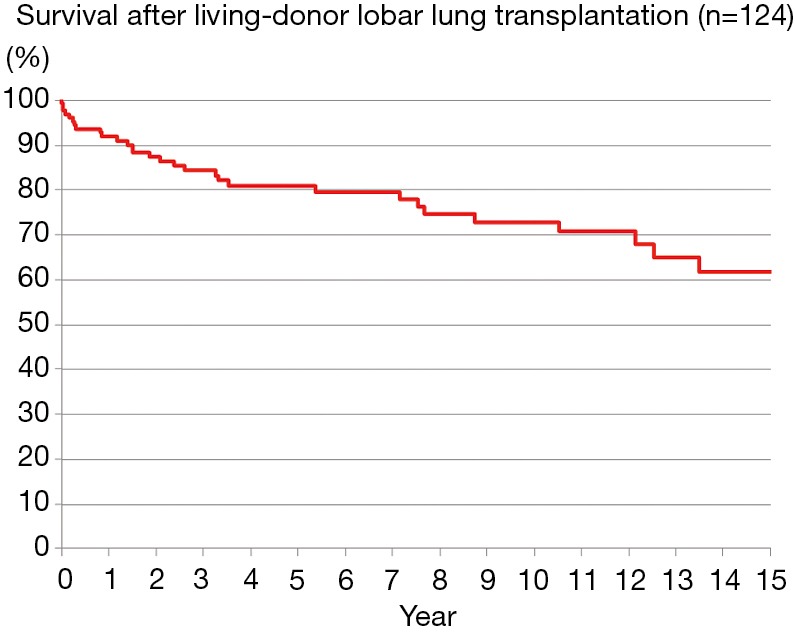
Living-donor lobar lung transplantation (LDLLT) was developed to deal with the severe shortage of brain dead door for patients who would not survive the long waiting period. In standard LDLLT, right and left lower lobes removed from two healthy donors are implanted into a recipient after right and left pneumonectomies using cardiopulmonary bypass (CPB). The number of LDLLT has decreased in the USA due to the recent change in allocation system for cadaveric donor lungs. For the past several years, most of the reports on LDLLT have been from Japan, where the average waiting time for a cadaveric lung is exceeding 800 days. LDLLT has been performed both for adult and pediatric patients suffering from various end-stage lung diseases including restrictive, obstructive, vascular and infectious lung diseases. Since only two lobes are implanted, size matching is a very important issue. Functional size matching by measuring donor pulmonary function and anatomical size matching by three-dimensional computed tomography (3D-CT) volumetry are very useful. For oversize graft, we have employed several techniques, including single lobe transplantation, delayed chest closure, downsizing the graft, and middle lobe transplantation. In cases of undersize mismatch, native upper lobe sparing transplant or right-left inverted transplant was performed. The 5-, 10- and 15-year survivals were 80.8%, 72.6% and 61.7%, respectively. There was no difference in survival between standard LDLLT and non-standard LDLLT such as single, sparing and inverted transplant. All donors have been discharged without any restrictions. LDLLT is a viable option for very ill patients who would not survive a long waiting time for cadaveric lungs. We have successfully developed various surgical techniques to overcome size mismatching with favorable outcome.
Keywords: Lung transplantation; cadaveric lung transplantation (CLT); living-donor lobar lung transplantation (LDLLT); size matching.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures
References
-
- Starnes VA, Lewiston NJ, Luikart H, et al. Current trends in lung transplantation. Lobar transplantation and expanded use of single lungs. J Thorac Cardiovasc Surg 1992;104:1060-5; discussion 1065-6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous