

Atypical carcinoid localized at the bronchus accompanied by diffuse idiopathic pulmonary neuroendocrine cell hyperplasia in the distal lung: a rare case report
- PMID: 29221341
- PMCID: PMC5708499
- DOI: 10.21037/jtd.2017.08.75
Atypical carcinoid localized at the bronchus accompanied by diffuse idiopathic pulmonary neuroendocrine cell hyperplasia in the distal lung: a rare case report
Abstract
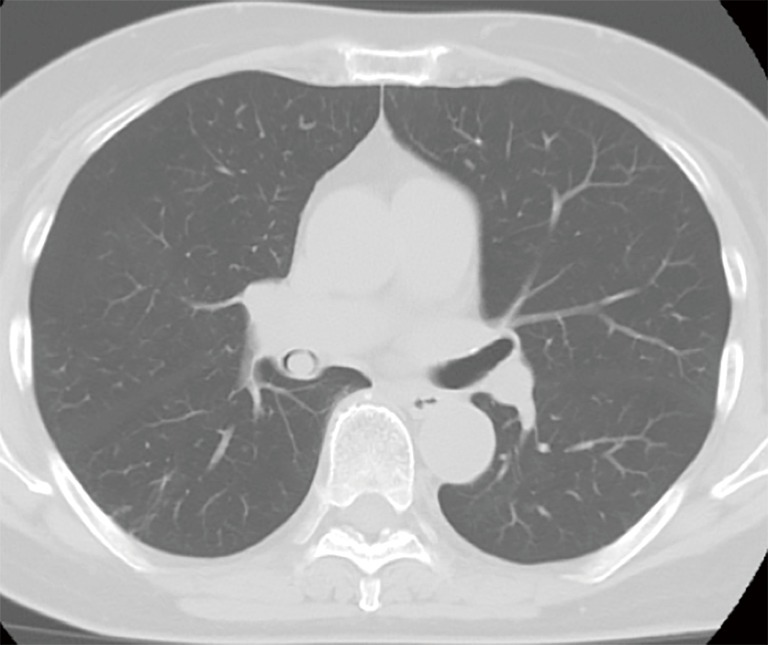
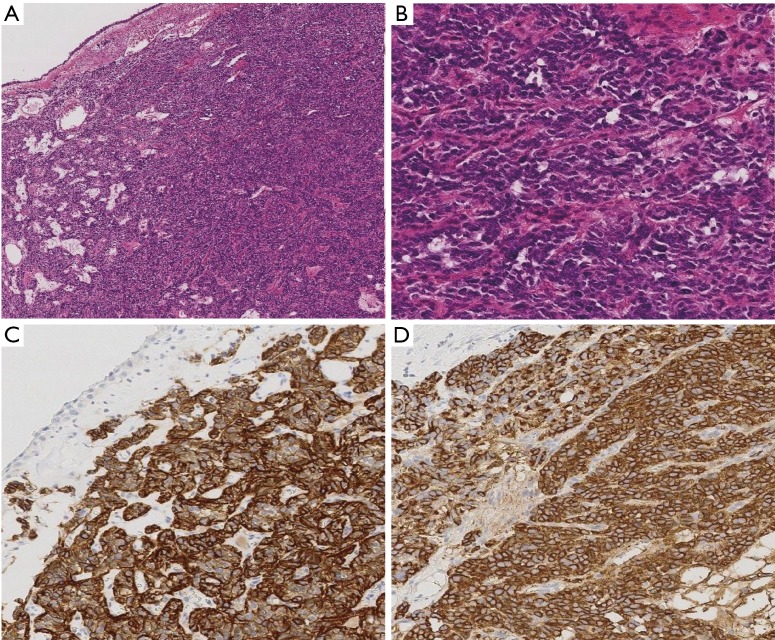
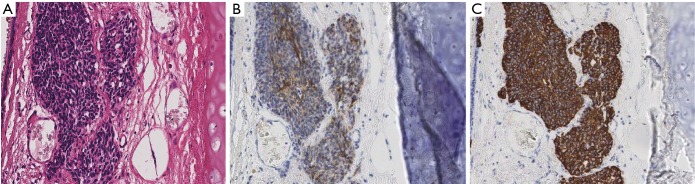
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH) is hyperplasia of noninvasive neuroendocrine cells originating from Kultchitsky cells. This is a rare pathological condition, suspected to be a precursor lesion of carcinoid, together with tumorlet. In the WHO histological classification (4th edition) revised in 2015, DIPNECH was added to the category that includes neuroendocrine tumors. Our patient was a 77-year-old woman who initially visited another doctor because of coughing. Chest CT revealed a mass occluding the right intermediate bronchial trunk, and bronchial carcinoid was suspected from biopsy findings, leading to referral of this patient to our department. The tumor was excised under a rigid bronchoscope for the purpose of making a definitive histological diagnosis and determining the extent of spread. The stalk portion of the tumor extended from the bifurcation of the middle and lower lobe bronchi in the membranous part of the intermediate trunk to the central side. The airway appeared to be almost completely occluded under bronchoscopy, but aeration from the periphery was maintained. Histopathologically, there was hyperplasia of oval atypical cells with relatively poor cytoplasm beneath the bronchial mucosa on HE staining, suggesting neuroendocrine tumor. Immunostaining revealed that these cells were positive for CD56, chromogranin A, and synaptophysin, and that there was moderate mitosis, leading to a diagnosis of atypical carcinoid. At a later date, radical surgery comprised of right pulmonary middle and lower lobectomy and lymph node dissection was performed. The final histopathological diagnosis was atypical carcinoid of the bronchus (pT1aN0M0, stage IA). There were multiple aggregations of atypical cells, measuring approximately 1-3 mm, along the airway around the bronchioles in the excised lung, indicating concomitant DIPNECH. The patient currently has no evidence of either recurrence or metastasis at 12 months after surgery, but we will continue meticulous follow-up.
Keywords: Atypical carcinoid; diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH); neuroendocrine tumors; rigid bronchoscope; tumorlet.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
A case of multiple lung carcinoid tumors localized in the right lower lobe.Respir Med Case Rep. 2022 May 27;38:101679. doi: 10.1016/j.rmcr.2022.101679. eCollection 2022. Respir Med Case Rep. 2022. PMID: 35656094 Free PMC article.
-
A Rare Case of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: A Case Report.Cureus. 2024 Jun 17;16(6):e62527. doi: 10.7759/cureus.62527. eCollection 2024 Jun. Cureus. 2024. PMID: 39022484 Free PMC article.
-
Lung carcinoid tumors with Diffuse Idiopathic Pulmonary NeuroEndocrine Cell Hyperplasia (DIPNECH) exhibit pejorative pathological features.Lung Cancer. 2021 Jun;156:117-121. doi: 10.1016/j.lungcan.2021.04.024. Epub 2021 Apr 30. Lung Cancer. 2021. PMID: 33940544
-
Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: Case series and a review of the literature.Medicine (Baltimore). 2018 Dec;97(52):e13806. doi: 10.1097/MD.0000000000013806. Medicine (Baltimore). 2018. PMID: 30593169 Free PMC article. Review.
-
Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: A Case Report and Review of the Literature.Am J Case Rep. 2017 Sep 11;18:975-979. doi: 10.12659/ajcr.904468. Am J Case Rep. 2017. PMID: 28890532 Free PMC article. Review.
Cited by
-
Rare diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: one case report and literature review.Transl Cancer Res. 2020 Dec;9(12):7657-7661. doi: 10.21037/tcr-20-1783. Transl Cancer Res. 2020. PMID: 35117365 Free PMC article.
References
-
- Shotsu A, Maehara T, Adachi H, et al. A Case of Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia with Peripheral Carcinoid Tumorlet. Haigan 2008;48:215-20. 10.2482/haigan.48.215 - DOI
-
- Fraser RS, Mulleret NL, Colman NC, et al. Neuroendocrine neoplasms. In: Fraser RS. editor. Fraser and Pare’s Diagnosis of Diseases of the Chest. Philadelphia: WB Saunders Co, 1999;1229-50.
-
- Arrigoni MG, Woolner LB, Bernatz PE. Atypical carcinoid tumors of the lung. J Thorac Cardiovasc Surg 1972;64:413-21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials