

Extracorporeal membrane oxygenation system as a bridge to reparative surgery in ventricular septal defect complicating acute inferoposterior myocardial infarction
- PMID: 29221351
- PMCID: PMC5708510
- DOI: 10.21037/jtd.2017.08.164
Extracorporeal membrane oxygenation system as a bridge to reparative surgery in ventricular septal defect complicating acute inferoposterior myocardial infarction
Abstract
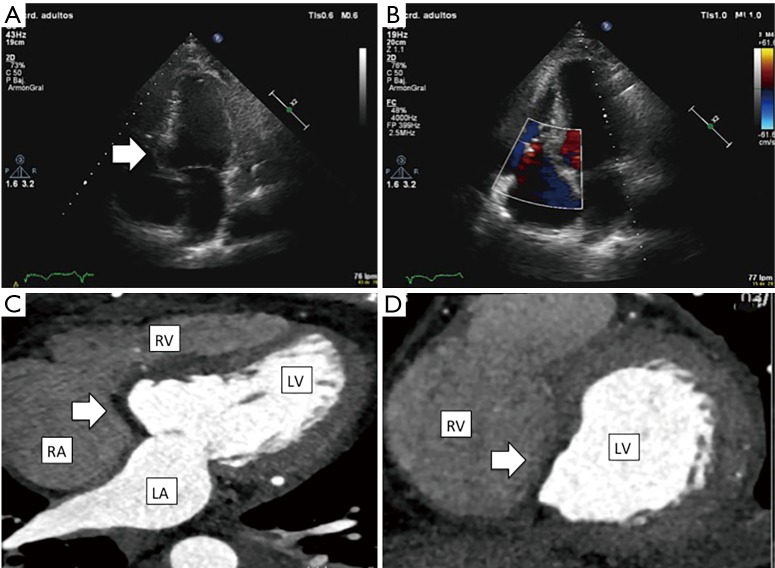
Post-infarction ventricular septal defect (VSD) is a rare but potentially lethal complication of acute myocardial infarction. Medical management is usually futile, so definitive surgery remains the treatment of choice but the risk surgery is very high and the optimal timing for surgery is still under debate. A 55-year-old man with no previous medical history attended the emergency-room for 12 h evolution of oppressive chest pain and strong anginal pain 7 days ago. On physical examination, blood pressure was 96/70 mmHg, pansystolic murmur over left sternal border without pulmonary crackles. An electrocardiogram revealed sinus rhythm 110 bpm, elevation ST and Q in inferior-posterior leads. Transthoracic echocardiogram showed inferoposterior akinesia, posterior-basal septal rupture (2 cm × 2 cm) with left-right shunt. Suspecting VSD in inferior-posterior acute myocardial infarction evolved, we performed emergency coronarography with 3-vessels disease and complete subacute occlusion of the mid segment of the right coronary artery. Left ventriculography demonstrated shunting of contrast from the left ventricule to the right ventricule. He was rejected for heart transplantation because of his age. Considering the high surgical risk to early surgery and his hemodynamic and clinical stability, delayed surgical treatment is decided, and 4 days after admission the patient suffered hemodynamic instability so venoarterial extracorporeal membrane oxygenation system (ECMO) is implanted as a bridge to reparative surgery. The 9th day after admission double bypass, interventricular defect repair with pericardial two-patch exclusion technique, and ECMO decannulation were performed. The patient's postoperative course was free of complications and was discharged 10 days post VSD repair surgery. Follow-up 3-month later revealed the patient to be in good functional status and good image outcome with intact interventricular septal patch without shunt. ECMO as a bridge to reparative surgery in postinfarction VSD is an adequate option to stabilize patients until surgery.
Keywords: Ventricular septal defect (VSD); extracorporeal membrane oxygenation system (ECMO); mechanical circulatory support; myocardial infarction.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources