

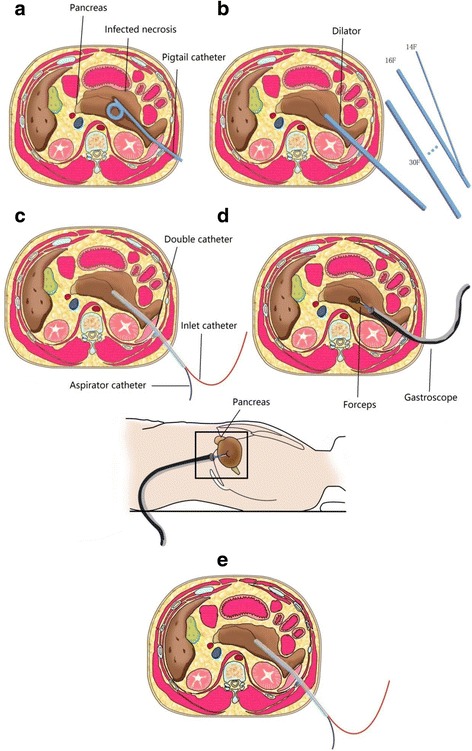
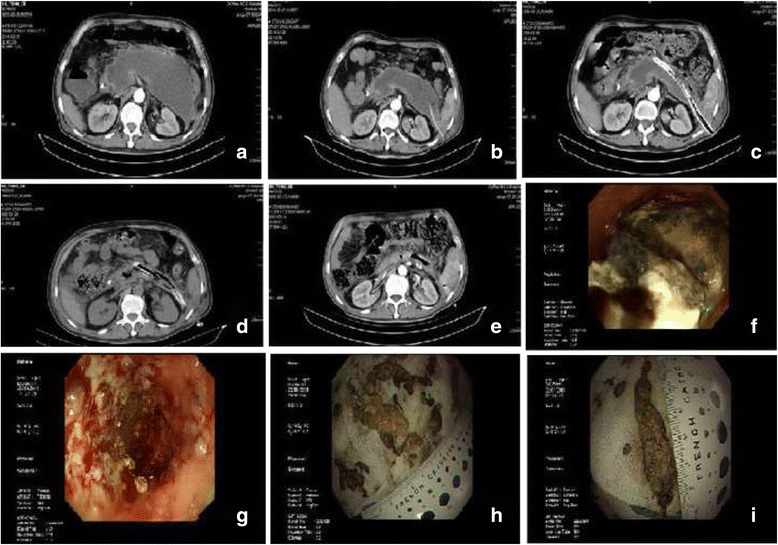
Double-catheter lavage combined with percutaneous flexible endoscopic debridement for infected pancreatic necrosis failed to percutaneous catheter drainage
- PMID: 29221438
- PMCID: PMC5723031
- DOI: 10.1186/s12876-017-0717-3
Double-catheter lavage combined with percutaneous flexible endoscopic debridement for infected pancreatic necrosis failed to percutaneous catheter drainage
Abstract
Background: Infected pancreatic necrosis (IPN) is a serious local complication of acute pancreatitis, with high mortality. Minimally invasive therapy including percutaneous catheter drainage (PCD) has become the preferred method for IPN instead of traditional open necrosectomy. However, the efficacy of double-catheter lavage in combination with percutaneous flexible endoscopic debridement after PCD failure is unknown compared with surgical necrosectomy.
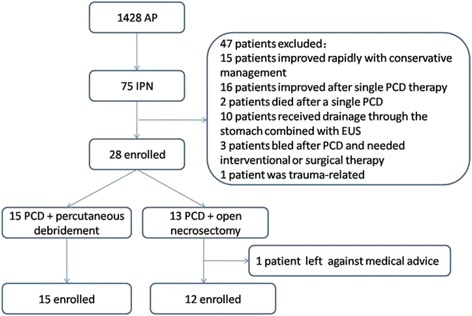
Methods: A total of 27 cases of IPN patients with failure PCD between Jan 2014 and Dec 2015 were enrolled in this retrospective cohort study. Fifteen patients received double-catheter lavage in combination with percutaneous flexible endoscopic debridement, and 12 patients underwent open necrosectomy. The primary endpoint was the composite end point of major complications or death. The secondary endpoint included mortality, major complication rate, ICU admission length of stay, and overall length of stay.
Results: The primary endpoint occurrence rate in double-catheter lavage in combination with percutaneous flexible endoscopic debridement group (8/15, 53%) was significantly lower than that in open necrosectomy group (11/12, 92%) (RR = 1.71, 95% CI = 1.04 - 2.84, P < 0.05). Though the mortality between two groups showed no statistical significance (0% vs. 17%, P = 0.19), the rate of new-onset multiple organ failure and ICU admission length of stay in the experimental group was significantly lower than that in open necrosectomy group (13% vs. 58%, P = 0.04; 0 vs. 17, P = 0.02, respectively). Only 40% of patients required ICU admission after percutaneous debridement, which was markedly lower than the patients who underwent surgery (83%; P < 0.05).
Conclusions: Double-catheter lavage in combination with percutaneous flexible endoscopic debridement showed superior effectiveness, safety, and convenience in patients with IPN after PCD failure as compared to open necrosectomy.
Keywords: Double-catheter lavage; Infected pancreatic necrosis; Open necrosectomy; Percutaneous catheter drainage; Percutaneous flexible endoscopic debridement.
Conflict of interest statement
Ethics approval and consent to participate
The Medical Ethics Committee of the First Affiliated Hospital of Nanchang University approved the protocol(Ethical approval No. 2013020). Each participant provided written informed consent to be included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Percutaneous Endoscopic Step-Up Therapy Is an Effective Minimally Invasive Approach for Infected Necrotizing Pancreatitis.Dig Dis Sci. 2020 Feb;65(2):615-622. doi: 10.1007/s10620-019-05696-2. Epub 2019 Jun 11. Dig Dis Sci. 2020. PMID: 31187325
-
American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis.Gastroenterology. 2020 Jan;158(1):67-75.e1. doi: 10.1053/j.gastro.2019.07.064. Epub 2019 Aug 31. Gastroenterology. 2020. PMID: 31479658 Review.
-
Comparison between minimally invasive and open surgical treatment in necrotizing pancreatitis.J Surg Res. 2017 Apr;210:22-31. doi: 10.1016/j.jss.2016.10.022. Epub 2016 Nov 2. J Surg Res. 2017. PMID: 28457332
-
[Four-steps surgery for infected pancreatic necrosis based on "Step-up" strategy: a retrospective study].Zhonghua Wai Ke Za Zhi. 2020 Nov 1;58(11):858-863. doi: 10.3760/cma.j.cn112139-20200429-00348. Zhonghua Wai Ke Za Zhi. 2020. PMID: 33120449 Chinese.
-
Combined endoscopic trangastric drainage and video assisted retroperitoneal pancreatic debridement - The best of both worlds for extensive pancreatic necrosis with enteric fistulae.Pancreatology. 2016 Sep-Oct;16(5):788-90. doi: 10.1016/j.pan.2016.06.009. Epub 2016 Jun 19. Pancreatology. 2016. PMID: 27344627 Review.
Cited by
-
Percutaneous endoscopic necrosectomy (PEN) for treatment of necrotizing pancreatitis: a systematic review and meta-analysis.Endosc Int Open. 2023 Mar 23;11(3):E258-E267. doi: 10.1055/a-1935-4738. eCollection 2023 Mar. Endosc Int Open. 2023. PMID: 36968976 Free PMC article.
-
Percutaneous Endoscopic Necrosectomy-A Review of the Literature.J Clin Med. 2022 Jul 6;11(14):3932. doi: 10.3390/jcm11143932. J Clin Med. 2022. PMID: 35887696 Free PMC article. Review.
-
Acute Necrotizing Pancreatitis-Advances and Challenges in Management for Optimal Clinical Outcomes.Medicina (Kaunas). 2025 Jun 30;61(7):1186. doi: 10.3390/medicina61071186. Medicina (Kaunas). 2025. PMID: 40731816 Free PMC article. Review.
-
Open necrosectomy combined with continuous positive drainage and prophylactic diverting loop ileostomy for late infected pancreatic necrosis: a retrospective cohort study.BMC Gastroenterol. 2020 Jul 8;20(1):212. doi: 10.1186/s12876-020-01343-7. BMC Gastroenterol. 2020. PMID: 32640995 Free PMC article.
-
Impact of continuous local lavage on pancreatic juice-related postoperative complications: Three case reports.World J Clin Cases. 2019 Sep 6;7(17):2526-2535. doi: 10.12998/wjcc.v7.i17.2526. World J Clin Cases. 2019. PMID: 31559288 Free PMC article.
References
-
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013;13:e1-15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
