

The impacts of baseline ventilator parameters on hospital mortality in acute respiratory distress syndrome treated with venovenous extracorporeal membrane oxygenation: a retrospective cohort study
- PMID: 29221484
- PMCID: PMC5723060
- DOI: 10.1186/s12890-017-0520-5
The impacts of baseline ventilator parameters on hospital mortality in acute respiratory distress syndrome treated with venovenous extracorporeal membrane oxygenation: a retrospective cohort study
Abstract
Background: Venovenous extracorporeal membrane oxygenation (VV-ECMO) is a valuable life support in acute respiratory distress syndrome (ARDS) in adult patients. However, the success of VV-ECMO is known to be influenced by the baseline settings of mechanical ventilation (MV) before its institution. This study was aimed at identifying the baseline ventilator parameters which were independently associated with hospital mortality in non-trauma patients receiving VV-ECMO for severe ARDS.
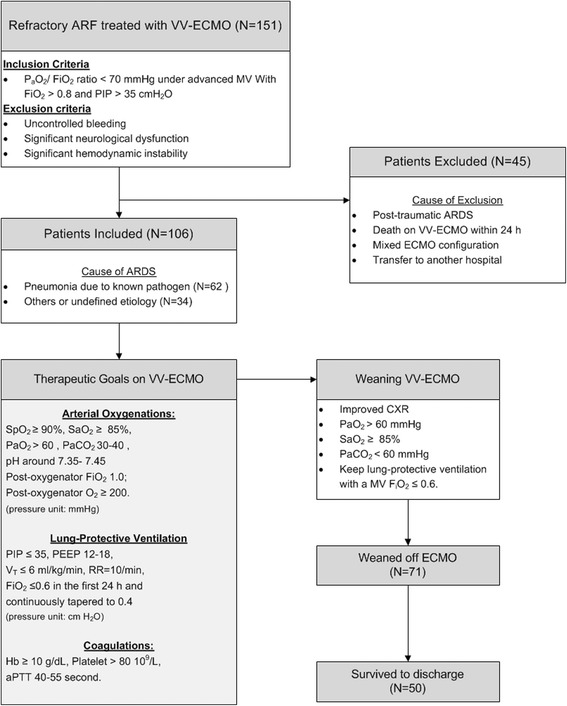
Methods: This retrospective study included 106 non-trauma patients (mean age: 53 years) who received VV-ECMO for ARDS in a single medical center from 2007 to 2016. The indication of VV-ECMO was severe hypoxemia (PaO2/ FiO2 ratio < 70 mmHg) under pressure-controlled MV with peak inspiratory pressure (PIP) > 35 cmH2O, positive end-expiratory pressure (PEEP) > 5 cmH2O, and FiO2 > 0.8. Important demographic and clinical data before and during VV-ECMO were collected for analysis of hospital mortality.
Results: The causes of ARDS were bacterial pneumonia (n = 41), viral pneumonia (n = 24), aspiration pneumonitis (n = 3), and others (n = 38). The median duration of MV before ECMO institution was 3 days and the overall hospital mortality was 53% (n = 56). The medians of PaO2/ FiO2 ratio, PIP, PEEP, and dynamic pulmonary compliance (PCdyn) at the beginning of MV were 84 mmHg, 32 cmH2O, 10 cmH2O, and 21 mL/cmH2O, respectively. However, before the beginning of VV-ECMO, the medians of PaO2/ FiO2 ratio, PIP, PEEP, and PCdyn became 69 mmHg, 36 cmH2O, 14 cmH2O, and 19 mL/cmH2O, respectively. The escalation of PIP and the declines in PaO2/ FiO2 ratio and PCdyn were significantly correlated with the duration of MV before ECMO institution. Finally, the duration of MV (OR: 1.184, 95% CI: 1.079-1.565, p < 0.001) was found to be the only baseline ventilator parameter that independently affected the hospital mortality in these ECMO-treated patients.
Conclusion: Since the duration of MV before ECMO institution was strongly correlated to the outcome of adult respiratory ECMO, medical centers are suggested to find a suitable prognosticating tool to determine the starting point of respiratory ECMO among their candidates with different duration of MV.
Trial registration: This study reported a health care intervention on human participants and was retrospectively registered. The Chang Gung Medical Foundation Institutional Review Board approved the study (no. 201601483B0 ) on November 23, 2016. All of the data were extracted from December 1, 2016, to January 31, 2017.
Keywords: Adult respiratory distress syndrome; Lung recruitment; Lung-protective mechanical ventilation; Venovenous extracorporeal membrane oxygenation.
Conflict of interest statement
Ethics approval and consent to participate
The Chang Gung Medical Foundation Institutional Review Board (no. 201601483B0) approved the study and waived the requirement for informed consent due to the retrospective nature of this study.
Consent for publication
Not applicable.
Competing interests
None of the authors have a conflict of interest to declare in relation to this work.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Venovenous Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome in Adults: Prognostic Factors for Outcomes.Medicine (Baltimore). 2016 Feb;95(8):e2870. doi: 10.1097/MD.0000000000002870. Medicine (Baltimore). 2016. PMID: 26937920 Free PMC article.
-
Is There a Preinterventional Mechanical Ventilation Time Limit for Candidates of Adult Respiratory Extracorporeal Membrane Oxygenation.ASAIO J. 2017 Sep/Oct;63(5):650-658. doi: 10.1097/MAT.0000000000000577. ASAIO J. 2017. PMID: 28525416
-
The impact of venovenous extracorporeal membrane oxygenation on cytokine levels in patients with severe acute respiratory distress syndrome: a prospective, observational study.Crit Care Resusc. 2017 Oct;19(Suppl 1):37-44. Crit Care Resusc. 2017. PMID: 29084500
-
Setting mechanical ventilation in ARDS patients during VV-ECMO: where are we?Minerva Anestesiol. 2015 Dec;81(12):1369-76. Epub 2014 Oct 10. Minerva Anestesiol. 2015. PMID: 25300627 Review.
-
Venovenous extracorporeal membrane oxygenation for acute respiratory distress syndrome: a systematic review and meta-analysis.Lancet Respir Med. 2019 Feb;7(2):163-172. doi: 10.1016/S2213-2600(18)30452-1. Epub 2019 Jan 11. Lancet Respir Med. 2019. PMID: 30642776
Cited by
-
Prognostic models for mortality risk in patients requiring ECMO.Intensive Care Med. 2023 Feb;49(2):131-141. doi: 10.1007/s00134-022-06947-z. Epub 2023 Jan 4. Intensive Care Med. 2023. PMID: 36600027 Free PMC article.
-
Low-Frequency Ventilation May Facilitate Weaning in Acute Respiratory Distress Syndrome Treated with Extracorporeal Membrane Oxygenation: A Randomized Controlled Trial.J Clin Med. 2024 Aug 27;13(17):5094. doi: 10.3390/jcm13175094. J Clin Med. 2024. PMID: 39274307 Free PMC article.
-
Defining and understanding the "extra-corporeal membrane oxygenation gap" in the veno-venous configuration: Timing and causes of death.Artif Organs. 2022 Mar;46(3):349-361. doi: 10.1111/aor.14058. Epub 2021 Sep 7. Artif Organs. 2022. PMID: 34494291 Free PMC article.
-
Bleeding and thrombotic events in adults supported with venovenous extracorporeal membrane oxygenation: an ELSO registry analysis.Intensive Care Med. 2022 Feb;48(2):213-224. doi: 10.1007/s00134-021-06593-x. Epub 2021 Dec 18. Intensive Care Med. 2022. PMID: 34921625 Free PMC article.
-
Contraindications to the Initiation of Veno-Venous ECMO for Severe Acute Respiratory Failure in Adults: A Systematic Review and Practical Approach Based on the Current Literature.Membranes (Basel). 2021 Jul 30;11(8):584. doi: 10.3390/membranes11080584. Membranes (Basel). 2021. PMID: 34436348 Free PMC article. Review.
References
-
- Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure V1.3. 2013. https://www.elso.org/resources/guidelines.aspx. Accessed 1 Jan 2017.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
