

Immune stealth-driven O2 serotype prevalence and potential for therapeutic antibodies against multidrug resistant Klebsiella pneumoniae
- PMID: 29222409
- PMCID: PMC5722860
- DOI: 10.1038/s41467-017-02223-7
Immune stealth-driven O2 serotype prevalence and potential for therapeutic antibodies against multidrug resistant Klebsiella pneumoniae
Abstract
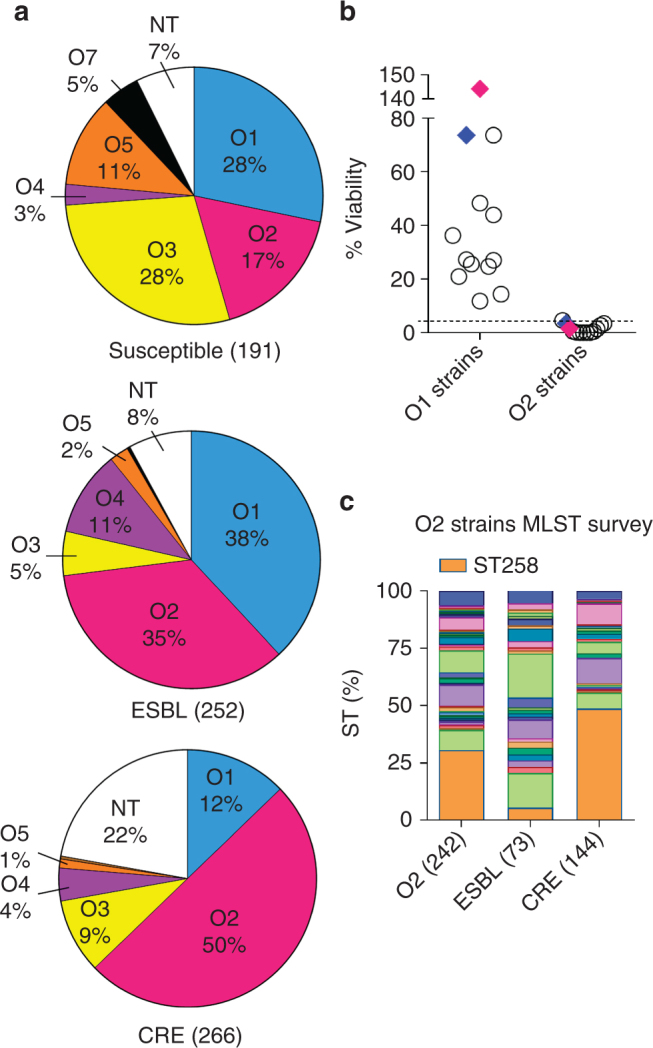
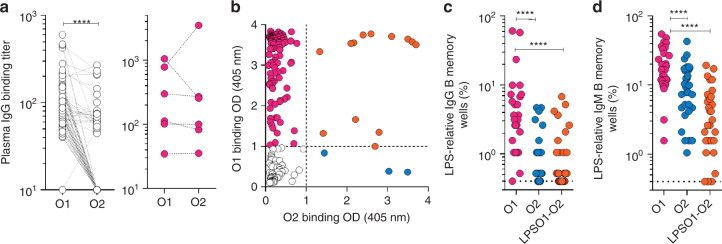
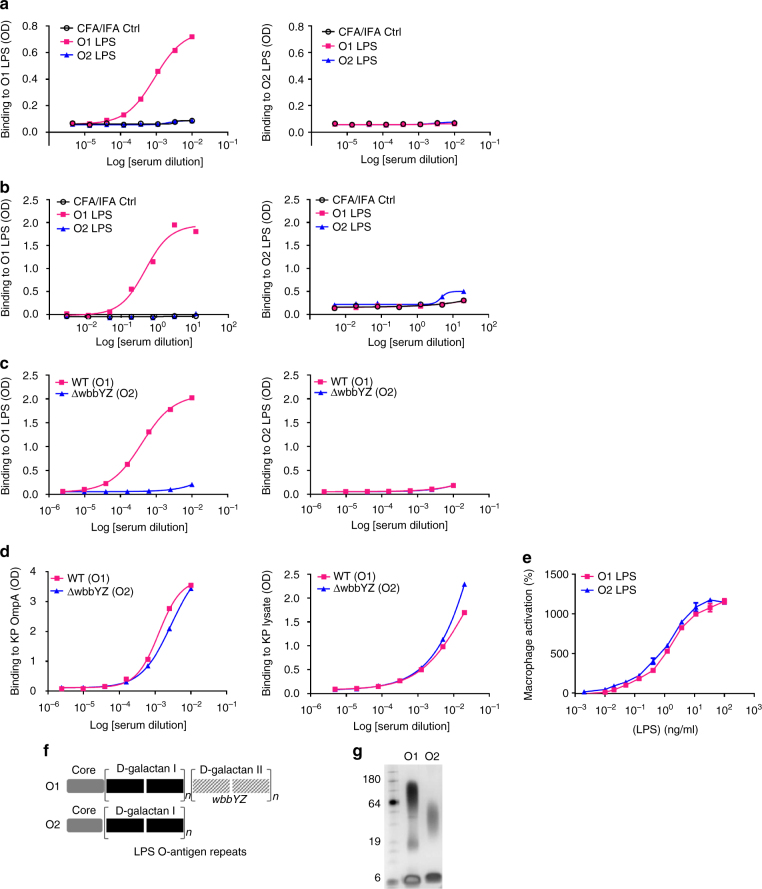
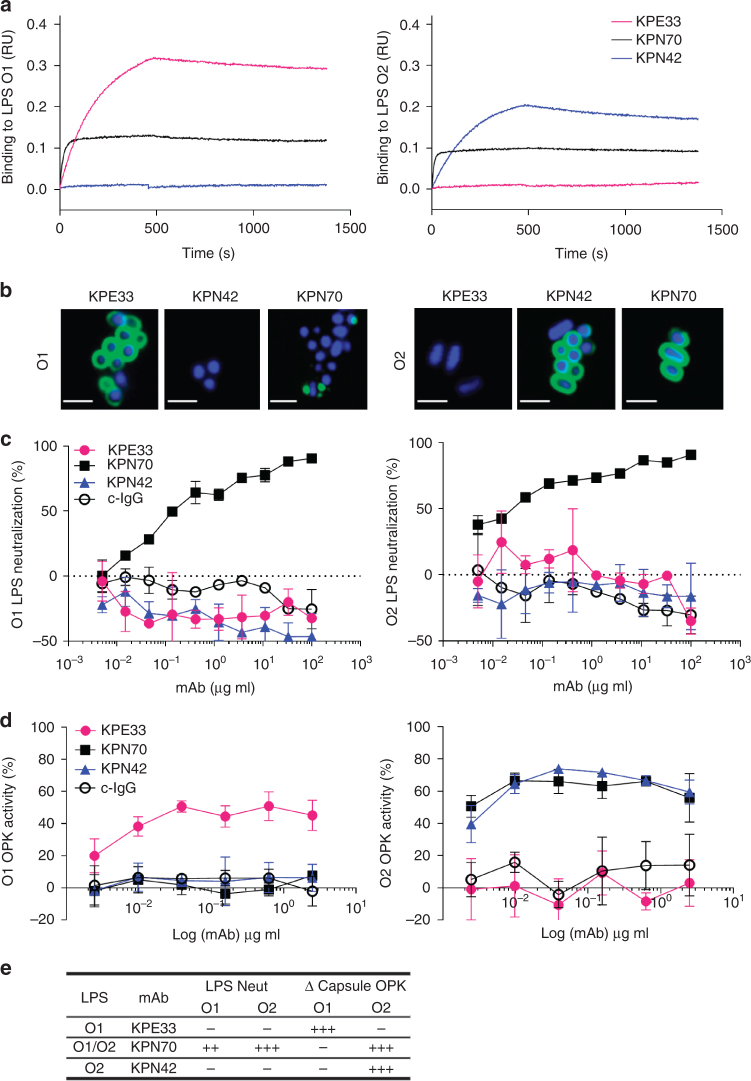
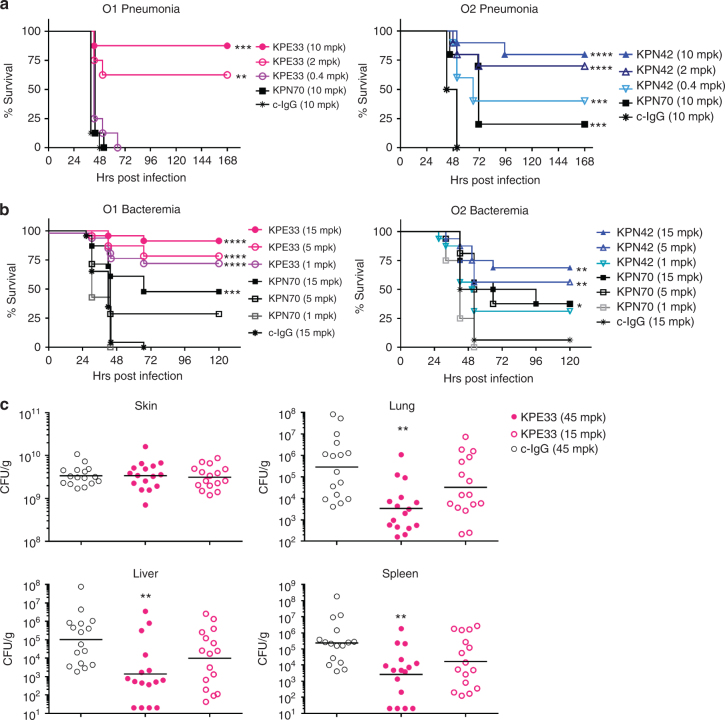
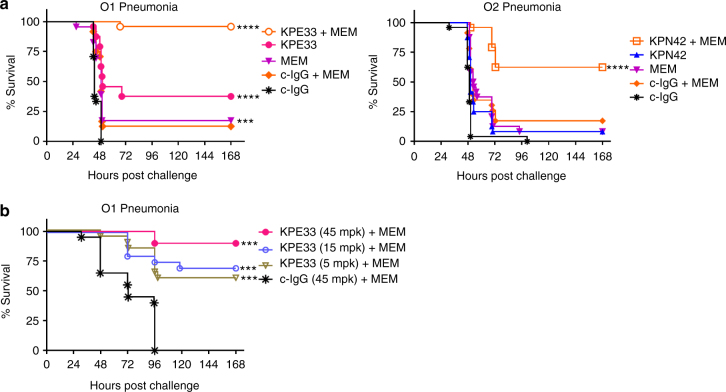
Emerging multidrug-resistant bacteria are a challenge for modern medicine, but how these pathogens are so successful is not fully understood. Robust antibacterial vaccines have prevented and reduced resistance suggesting a pivotal role for immunity in deterring antibiotic resistance. Here, we show the increased prevalence of Klebsiella pneumoniae lipopolysaccharide O2 serotype strains in all major drug resistance groups correlating with a paucity of anti-O2 antibodies in human B cell repertoires. We identify human monoclonal antibodies to O-antigens that are highly protective in mouse models of infection, even against heavily encapsulated strains. These antibodies, including a rare anti-O2 specific antibody, synergistically protect against drug-resistant strains in adjunctive therapy with meropenem, a standard-of-care antibiotic, confirming the importance of immune assistance in antibiotic therapy. These findings support an antibody-based immunotherapeutic strategy even for highly resistant K. pneumoniae infections, and underscore the effect humoral immunity has on evolving drug resistance.
Conflict of interest statement
M.E.P., Q.W., M.P.,J.B, R.C, E.S, X.X, W.Z., M.M.C., A.D., P.W., J.S., C.K.S. are current or former employees of MedImmune/AstraZeneca and may own stock or stock options in the company. Patents describing the activity of the antibodies in this work have been filed by MedImmune. A.D.M., M.B, E.C., S.B, F.Z, A.L, D.C. are employees of HumAbs BioMed and may currently hold Humabs stocks or stock options. The remaining authors declare no competing financial interests.
Figures
References
-
- Badal RE, et al. Etiology, extended-spectrum beta-lactamase rates and antimicrobial susceptibility of Gram-negative bacilli causing intra-abdominal infections in patients in general pediatric and pediatric intensive care units--global data from the Study for Monitoring Antimicrobial Resistance Trends 2008 to 2010. Pediatr. Infect. Dis. J. 2013;32:636–640. doi: 10.1097/INF.0b013e3182886377. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
