

Transplanting hepatitis C virus-positive livers into hepatitis C virus-negative patients with preemptive antiviral treatment: A modeling study
- PMID: 29222916
- PMCID: PMC5991982
- DOI: 10.1002/hep.29723
Transplanting hepatitis C virus-positive livers into hepatitis C virus-negative patients with preemptive antiviral treatment: A modeling study
Abstract
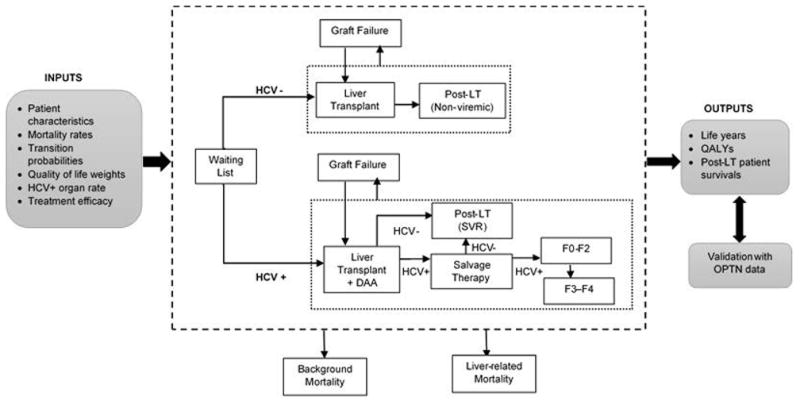
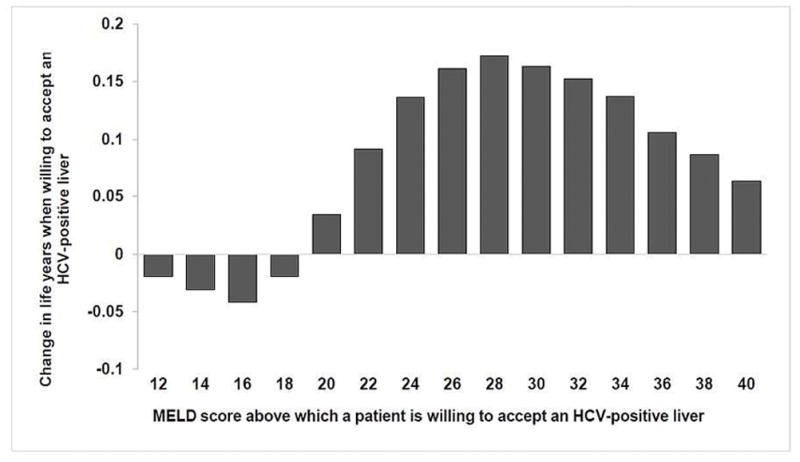
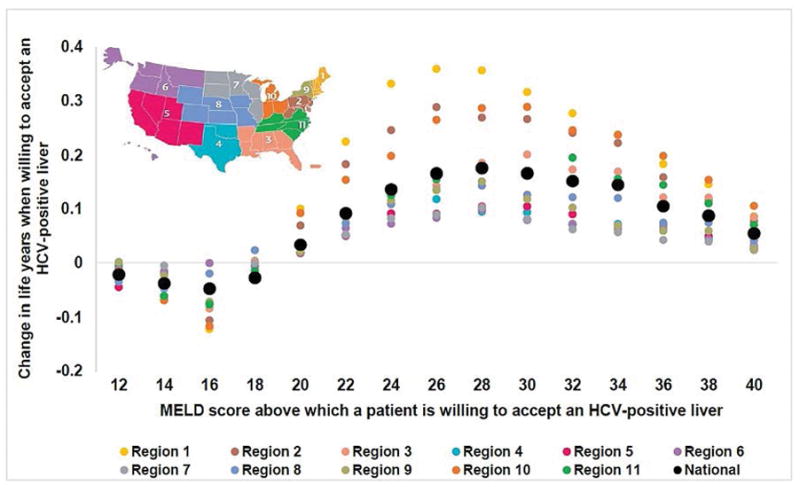
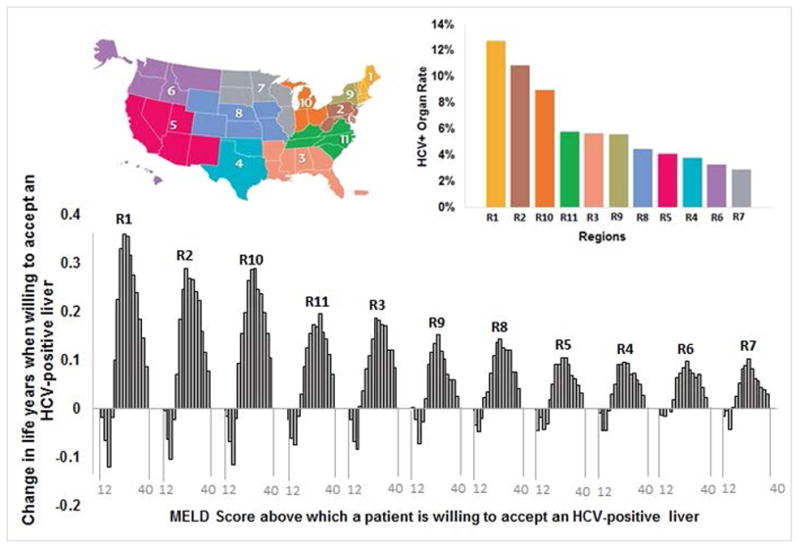
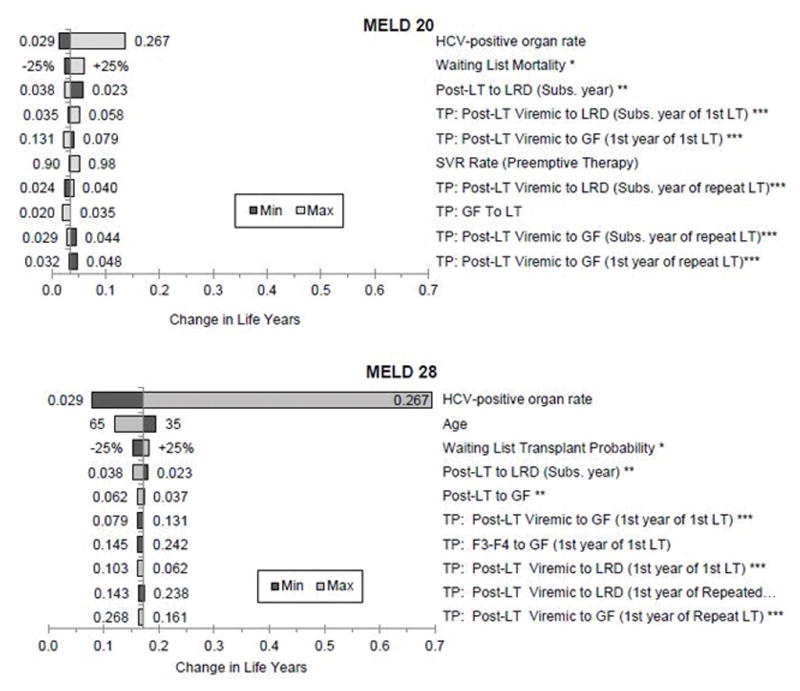
Under current guidelines, hepatitis C virus (HCV)-positive livers are not transplanted into HCV-negative recipients because of adverse posttransplant outcomes associated with allograft HCV infection. However, HCV can now be cured post-LT (liver transplant) using direct-acting antivirals (DAAs) with >90% success; therefore, HCV-negative patients on the LT waiting list may benefit from accepting HCV-positive organs with preemptive treatment. Our objective was to evaluate whether and in which HCV-negative patients the potential benefit of accepting an HCV-positive (i.e., viremic) organ outweighed the risks associated with HCV allograft infection. We developed a Markov-based mathematical model that simulated a virtual trial of HCV-negative patients on the LT waiting list to compare long-term outcomes in patients: (1) willing to accept any (HCV-negative or HCV-positive) liver versus (2) those willing to accept only HCV-negative livers. Patients receiving HCV-positive livers were treated preemptively with 12 weeks of DAA therapy and had a higher risk of graft failure than those receiving HCV-negative livers. The model incorporated data from published studies and the United Network for Organ Sharing (UNOS). We found that accepting any liver regardless of HCV status versus accepting only HCV-negative livers resulted in an increase in life expectancy when Model for End-Stage Liver Disease (MELD) was ≥20, and the benefit was highest at MELD 28 (0.172 additional life-years). The magnitude of clinical benefit was greater in UNOS regions with higher HCV-positive donor organ rates, that is, Regions 1, 2, 3, 10, and 11. Sensitivity analysis demonstrated that model outcomes were robust.
Conclusion: Transplanting HCV-positive livers into HCV-negative patients with preemptive DAA therapy could improve patient survival on the LT waiting list. Our analysis can help inform clinical trials and minimize patient harm. (Hepatology 2018;67:2085-2095).
© 2017 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Reply.Hepatology. 2018 Aug;68(2):793. doi: 10.1002/hep.30042. Hepatology. 2018. PMID: 29672882 No abstract available.
-
Expanding Donor Pool for Liver Transplantation by Utilizing Hepatitis C Virus-Infected Donors for Uninfected Recipients.Hepatology. 2018 Aug;68(2):792-793. doi: 10.1002/hep.30043. Hepatology. 2018. PMID: 29672899 Free PMC article. No abstract available.
References
-
- Kim WR, Lake JR, Smith JM, Skeans MA, Schladt DP, Edwards EB, Harper AM, et al. OPTN/SRTR 2015 Annual Data Report: Liver. Am J Transplant. 2017;17(Suppl 1):174–251. - PubMed
-
- Levitsky J, Formica RN, Bloom RD, Charlton M, Curry M, Friedewald J, Friedman J, et al. The American Society of Transplantation Consensus Conference on the Use of Hepatitis C Viremic Donors in Solid Organ Transplantation. American Journal of Transplantation. n/a-n/a. - PubMed
-
- Northup PG, Argo CK, Nguyen DT, McBride MA, Kumer SC, Schmitt TM, Pruett TL. Liver allografts from hepatitis C positive donors can offer good outcomes in hepatitis C positive recipients: a US National Transplant Registry analysis. Transpl Int. 2010;23:1038–1044. - PubMed
-
- Berenguer M, Prieto M, Rayon JM, Mora J, Pastor M, Ortiz V, Carrasco D, et al. Natural history of clinically compensated hepatitis C virus-related graft cirrhosis after liver transplantation. Hepatology. 2000;32:852–858. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
