

Atrial fibrillation decision support tool: Population perspective
- PMID: 29223435
- PMCID: PMC5726779
- DOI: 10.1016/j.ahj.2017.08.016
Atrial fibrillation decision support tool: Population perspective
Abstract
Background: Appropriate thromboprophylaxis for patients with atrial fibrillation or atrial flutter (AF) remains a national challenge. The recent availability of direct oral anticoagulants (DOACs) with comparable efficacy and improved safety compared with warfarin alters the balance between risk factors for stroke and benefit of anticoagulation. Our objective was to examine the impact of DOACs as an alternative to warfarin on the net benefit of oral anticoagulant therapy (OAT) in a real-world population of AF patients.
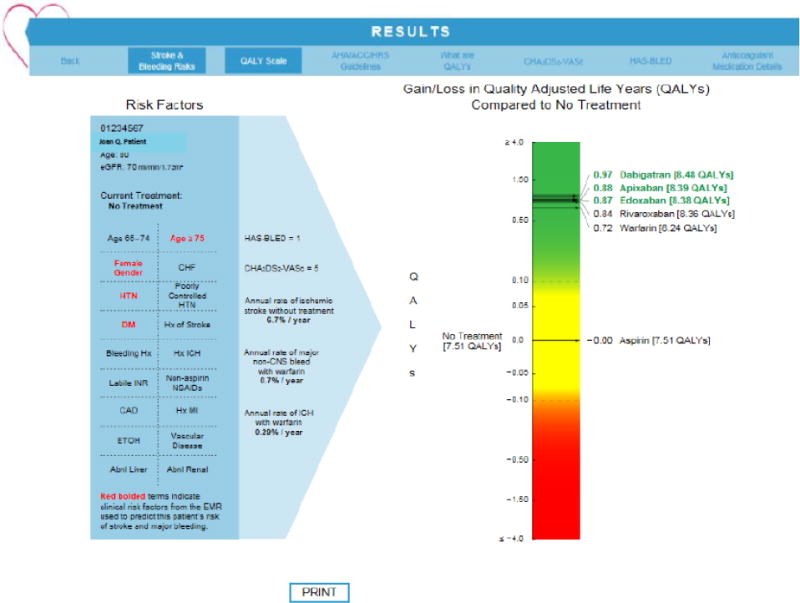
Methods: This is a retrospective cohort study of patients with paroxysmal or persistent nonvalvular AF. We updated an Atrial Fibrillation Decision Support Tool (AFDST) to include DOACs as treatment options. The tool generates patient-specific recommendations based upon individual patient risk factor profiles for stroke and major bleeding using quality-adjusted life-years (QALYs) calculated for each treatment strategy by a decision analytic model. The setting included inpatient and ambulatory sites in an academic health center in the midwestern United States. The study involved 5,121 adults with nonvalvular AF seen for any ambulatory visit or inpatient hospitalization over the 1-year period (January through December 2016). Outcome measure was net clinical benefit in QALYs.
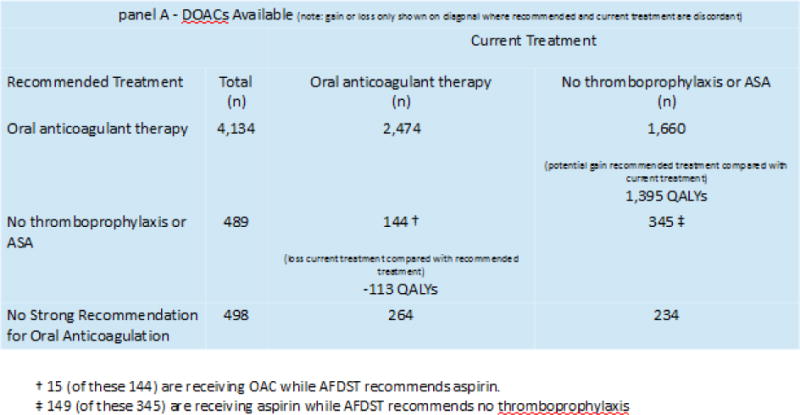
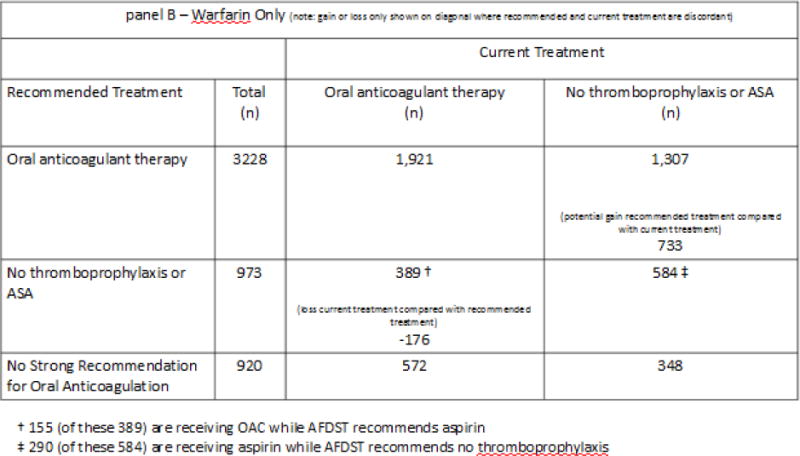
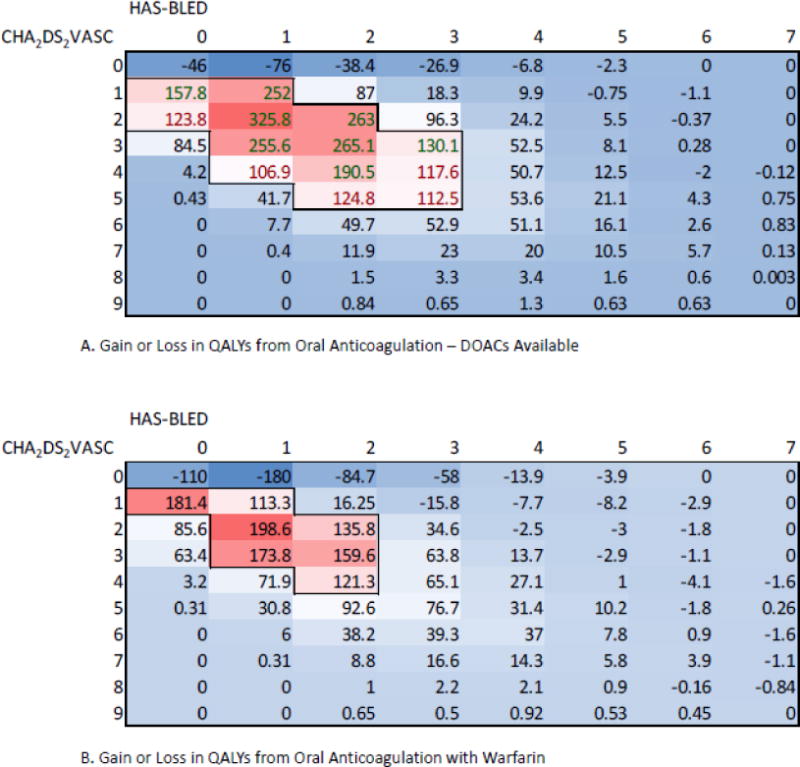
Results: When DOACs are a therapeutic option, the AFDST recommends OAT for 4,134 (81%) patients and no antithrombotic therapy or aspirin for 489 (9%). A strong recommendation for OAT could not be made in 498 (10%) patients. When warfarin is the only option, OAT is recommended for 3,228 (63%) patients and no antithrombotic therapy or aspirin for 973 (19%). A strong recommendation for OAT could not be made in 920 (18%) patients. In total, 1,508 QALYs could be gained if treatment were changed to that recommended by the AFDST.
Conclusions: Availability of DOACs increases the proportion of patients for whom oral anticoagulation therapy is recommended in a real-world cohort of AF patients and increased projected QALYs by more than 1,500 when all patients are receiving thromboprophylaxis as recommended by the AFDST compared with current treatment.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors report no conflicts.
Figures
References
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137:263–272. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
