

The global burden of tuberculosis: results from the Global Burden of Disease Study 2015
- PMID: 29223583
- PMCID: PMC5831985
- DOI: 10.1016/S1473-3099(17)30703-X
The global burden of tuberculosis: results from the Global Burden of Disease Study 2015
Abstract
Background: An understanding of the trends in tuberculosis incidence, prevalence, and mortality is crucial to tracking of the success of tuberculosis control programmes and identification of remaining challenges. We assessed trends in the fatal and non-fatal burden of tuberculosis over the past 25 years for 195 countries and territories.
Methods: We analysed 10 691 site-years of vital registration data, 768 site-years of verbal autopsy data, and 361 site-years of mortality surveillance data using the Cause of Death Ensemble model to estimate tuberculosis mortality rates. We analysed all available age-specific and sex-specific data sources, including annual case notifications, prevalence surveys, and estimated cause-specific mortality, to generate internally consistent estimates of incidence, prevalence, and mortality using DisMod-MR 2.1, a Bayesian meta-regression tool. We assessed how observed tuberculosis incidence, prevalence, and mortality differed from expected trends as predicted by the Socio-demographic Index (SDI), a composite indicator based on income per capita, average years of schooling, and total fertility rate. We also estimated tuberculosis mortality and disability-adjusted life-years attributable to the independent effects of risk factors including smoking, alcohol use, and diabetes.
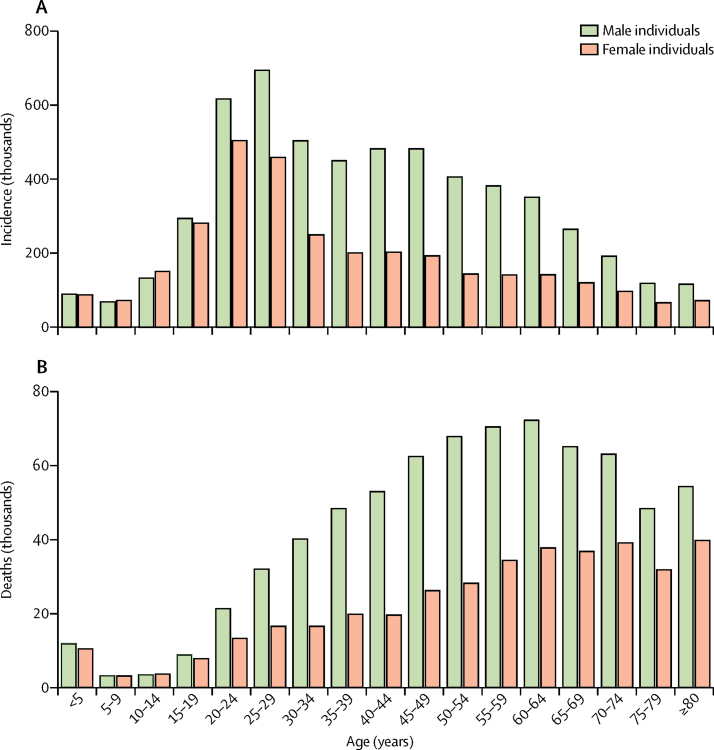
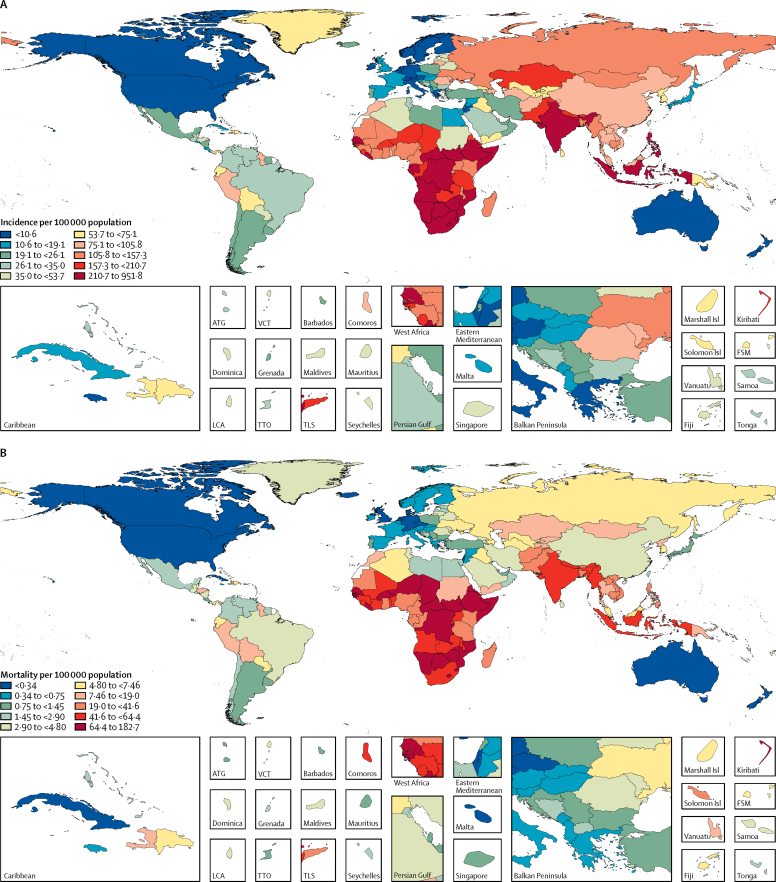
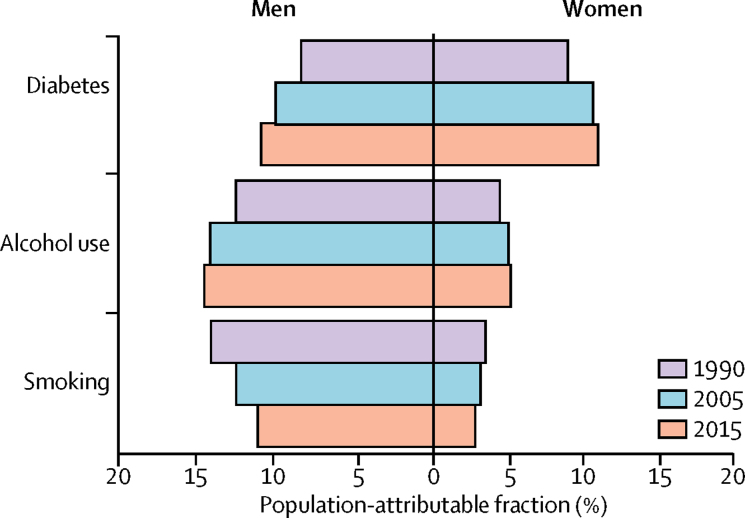
Findings: Globally, in 2015, the number of tuberculosis incident cases (including new and relapse cases) was 10·2 million (95% uncertainty interval 9·2 million to 11·5 million), the number of prevalent cases was 10·1 million (9·2 million to 11·1 million), and the number of deaths was 1·3 million (1·1 million to 1·6 million). Among individuals who were HIV negative, the number of incident cases was 8·8 million (8·0 million to 9·9 million), the number of prevalent cases was 8·9 million (8·1 million to 9·7 million), and the number of deaths was 1·1 million (0·9 million to 1·4 million). Annualised rates of change from 2005 to 2015 showed a faster decline in mortality (-4·1% [-5·0 to -3·4]) than in incidence (-1·6% [-1·9 to -1·2]) and prevalence (-0·7% [-1·0 to -0·5]) among HIV-negative individuals. The SDI was inversely associated with HIV-negative mortality rates but did not show a clear gradient for incidence and prevalence. Most of Asia, eastern Europe, and sub-Saharan Africa had higher rates of HIV-negative tuberculosis burden than expected given their SDI. Alcohol use accounted for 11·4% (9·3-13·0) of global tuberculosis deaths among HIV-negative individuals in 2015, diabetes accounted for 10·6% (6·8-14·8), and smoking accounted for 7·8% (3·8-12·0).
Interpretation: Despite a concerted global effort to reduce the burden of tuberculosis, it still causes a large disease burden globally. Strengthening of health systems for early detection of tuberculosis and improvement of the quality of tuberculosis care, including prompt and accurate diagnosis, early initiation of treatment, and regular follow-up, are priorities. Countries with higher than expected tuberculosis rates for their level of sociodemographic development should investigate the reasons for lagging behind and take remedial action. Efforts to prevent smoking, alcohol use, and diabetes could also substantially reduce the burden of tuberculosis.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Tuberculosis eradication: renewed commitment and global investment required.Lancet Infect Dis. 2018 Mar;18(3):228-229. doi: 10.1016/S1473-3099(17)30692-8. Epub 2017 Dec 7. Lancet Infect Dis. 2018. PMID: 29223584 No abstract available.
References
-
- US Agency for International Development Independent assessment of national TB prevalence surveys conducted between 2009–2015. February, 2016. https://www.usaid.gov/sites/default/files/documents/1864/TB-prevalence-s... (accessed Sept 30, 2016).
-
- WHO . World Health Organization; Geneva: 2016. Global tuberculosis report 2016.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
