

Residual Risk of Atherosclerotic Cardiovascular Events in Relation to Reductions in Very-Low-Density Lipoproteins
- PMID: 29223956
- PMCID: PMC5779048
- DOI: 10.1161/JAHA.117.007402
Residual Risk of Atherosclerotic Cardiovascular Events in Relation to Reductions in Very-Low-Density Lipoproteins
Abstract
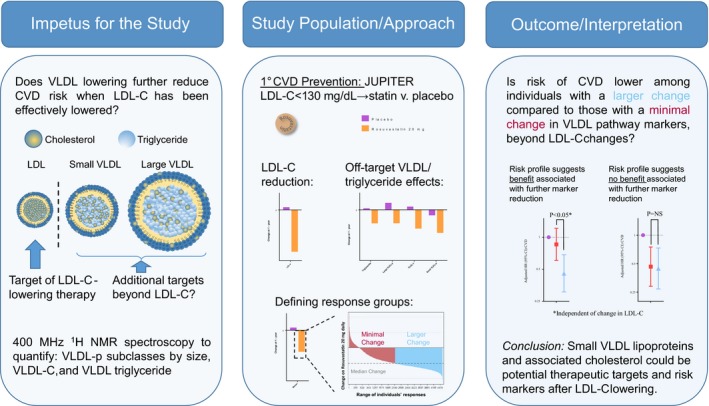
Background: It is uncertain whether pharmacological reductions in very-low-density lipoproteins (VLDLs), and their component triglyceride and cholesterol could reduce residual risk of atherosclerotic cardiovascular disease (ASCVD) events among individuals in whom low-density lipoprotein cholesterol (LDL-C) has been adequately lowered. We examined whether individuals with greater on-statin reductions in VLDL-related measures-beyond reductions in LDL-C-were at further reduced risk of ASCVD.
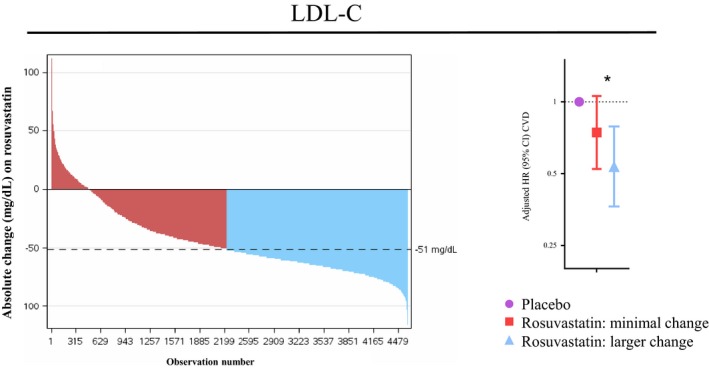
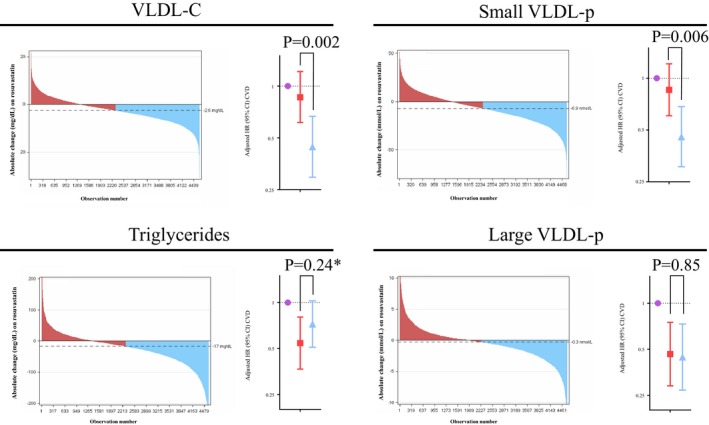
Methods and results: In 9423 participants in the JUPITER (Justification for the Use of Statins in Prevention) trial (NCT00239681), at baseline and on statin we measured standard lipids, 400-MHz proton nuclear magnetic resonance spectroscopy-measured VLDL particle subclasses (small, medium, and large VLDL lipoprotein particle concentration), and total VLDL cholesterol mass. Compared with individuals allocated to placebo, we examined risk of incident ASCVD (N=211) among statin-allocated participants who achieved minimal (<median) or greater (≥median) marker reductions using adjusted Cox models. On-statin changes in VLDL-related markers were only modestly correlated (Spearman r≤0.29) with change in LDL-C. On-statin median LDL-C was 54 mg/dL and triglyceride was 101 mg/dL. Dose-response reductions in ASCVD risk were observed for greater reductions in LDL-C, VLDL cholesterol mass, and small VLDL lipoprotein particle concentration; the latter 2 remained significant after incremental adjustment for change in LDL-C (P≤0.006). Conversely, there was no further risk reduction with greater reductions in triglycerides or large/medium VLDL lipoprotein particle concentration.
Conclusions: Pharmacological reduction in small, cholesterol-enriched, triglyceride-depleted VLDL was associated with reduction in ASCVD risk. Chemically measured triglycerides may not sufficiently capture risk related to VLDL pathways. These findings also support broader profiling of lipid and lipoprotein changes in response to statins as prognostic markers of individual benefit, supporting more precision-medicine, individualized approaches to cardiovascular risk reduction.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00239681.
Keywords: arteriosclerosis; lipids; lipoproteins; metabolomics; personalized medicine; primary prevention; statin.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Carroll MD, Kit BK, Lacher DA, Shero ST, Mussolino ME. Trends in lipids and lipoproteins in US adults, 1988–2010. JAMA. 2012;308:1545–1554. - PubMed
-
- Kuklina EV, Yoon PW, Keenan NL. Trends in high levels of low‐density lipoprotein cholesterol in the United States, 1999–2006. JAMA. 2009;302:2104–2110. - PubMed
-
- Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R, Collins R, Simes R; Cholesterol Treatment Trialists’ (CTT) Collaborators . Efficacy and safety of cholesterol‐lowering treatment: prospective meta‐analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- Rosenson RS, Davidson MH, Hirsh BJ, Kathiresan S, Gaudet D. Genetics and causality of triglyceride‐rich lipoproteins in atherosclerotic cardiovascular disease. J Am Coll Cardiol. 2014;64:2525–2540. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
