

Metabolic surgery for the treatment of type 2 diabetes in obese individuals
- PMID: 29224190
- PMCID: PMC6448954
- DOI: 10.1007/s00125-017-4513-y
Metabolic surgery for the treatment of type 2 diabetes in obese individuals
Abstract
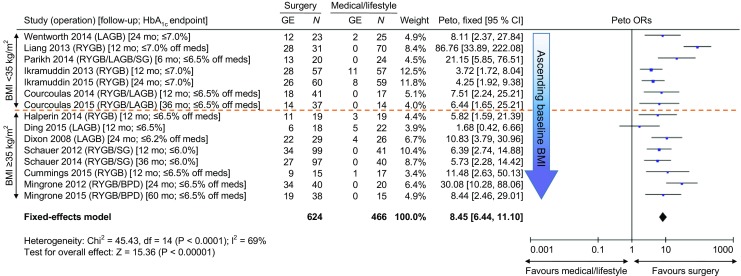
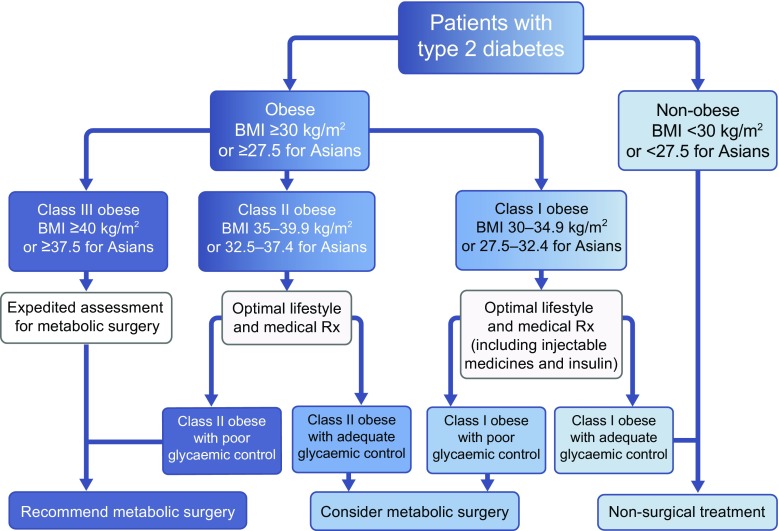
Several bariatric operations originally designed to promote weight loss have been found to powerfully treat type 2 diabetes, causing remission in most cases, through diverse mechanisms additional to the secondary consequences of weight loss. These observations have prompted consideration of such operations as 'metabolic surgery', used expressly to treat diabetes, including among patients who are only mildly obese or merely overweight. Large, long-term observational studies consistently demonstrate that bariatric/metabolic surgery is associated with reductions in all cardiovascular risk factors, actual cardiovascular events, microvascular diabetes complications, cancer and death. Numerous recent randomised clinical trials, directly comparing various surgical vs non-surgical interventions for diabetes, uniformly demonstrate the former to be superior for improvements in all glycaemic variables, as well as other metabolic endpoints. These benefits are similar among individuals with type 2 diabetes and a preoperative BMI of 30-35 kg/m2 compared with traditional bariatric surgery patients with a BMI >35 kg/m2. The safety profiles of modern laparoscopic bariatric/metabolic operations are similar to those of elective laparoscopic hysterectomy and knee arthroplasty. However, more evidence regarding the risks, benefits and costs of surgery is needed from very long-term (>5 year) randomised clinical trials powered to observe 'hard' clinical endpoints following the operations most commonly used today. Given the efficacy, safety and cost-effectiveness of metabolic surgery, the second Diabetes Surgery Summit (DSS-II) consensus conference recently placed surgery squarely within the overall diabetes treatment algorithm, recommending consideration of this approach for patients with inadequately controlled diabetes and a BMI as low as 30 kg/m2, or 27.5 kg/m2 for Asian individuals. These new guidelines have been formally ratified by 53 leading diabetes and surgery societies worldwide. Given this broad level of endorsement, we feel that the DSS-II recommendations should now replace the outdated National Institutes of Health (NIH) suggestions that have governed bariatric surgery practice and insurance compensation worldwide since 1991.
Keywords: Bariatric surgery; Biliopancreatic diversion; Diabetes Surgery Summit; Gastric bypass; Ghrelin; Glucagon-like peptide-1; Laparoscopic adjustable gastric banding; Metabolic surgery; Review; Vertical sleeve gastrectomy.
Conflict of interest statement
Duality of interest
DEC is a principal investigator on the Comparison of Surgery vs Medicine for Indian Diabetes (COSMID) randomised clinical trial, which is funded by Johnson & Johnson, as well as the Alliance of Randomized Trials of Medicine vs Metabolic Surgery in Type 2 Diabetes (ARMMS-T2D) randomised clinical trial, which has previously been sponsored in part by Johnson & Johnson plus Covidien, but is now fully funded by the NIH. FR declares that there is no duality of interest associated with this manuscript.
Contribution statement
DEC drafted the manuscript, and both authors revised it critically for important intellectual content. Both authors approved the version to be published.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
