

Role of Surgery in the Treatment of Masaoka Stage IVa Thymoma
- PMID: 29225302
- PMCID: PMC5833134
- DOI: 10.5761/atcs.oa.17-00108
Role of Surgery in the Treatment of Masaoka Stage IVa Thymoma
Abstract
Purpose: To analyze the role of surgery in patients with Masaoka stage IVa thymoma treated with multimodality therapy.
Methods: Of 191 patients undergoing surgery for thymoma in our department between January 2002 and December 2015, 39 (20.4%) had Masaoka stage IVa. Histopathological tumor type, myasthenic status of the Osserman-Genkins score, Masaoka stage at the first surgery, neoadjuvant treatment, number and type of surgeries, and survival rates were recorded.
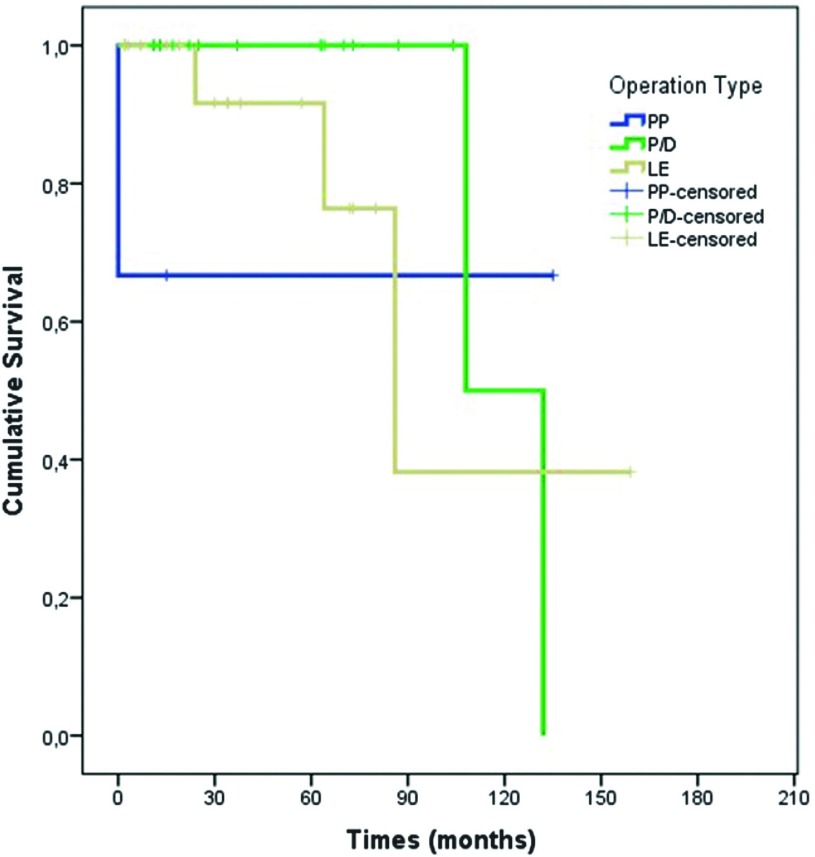
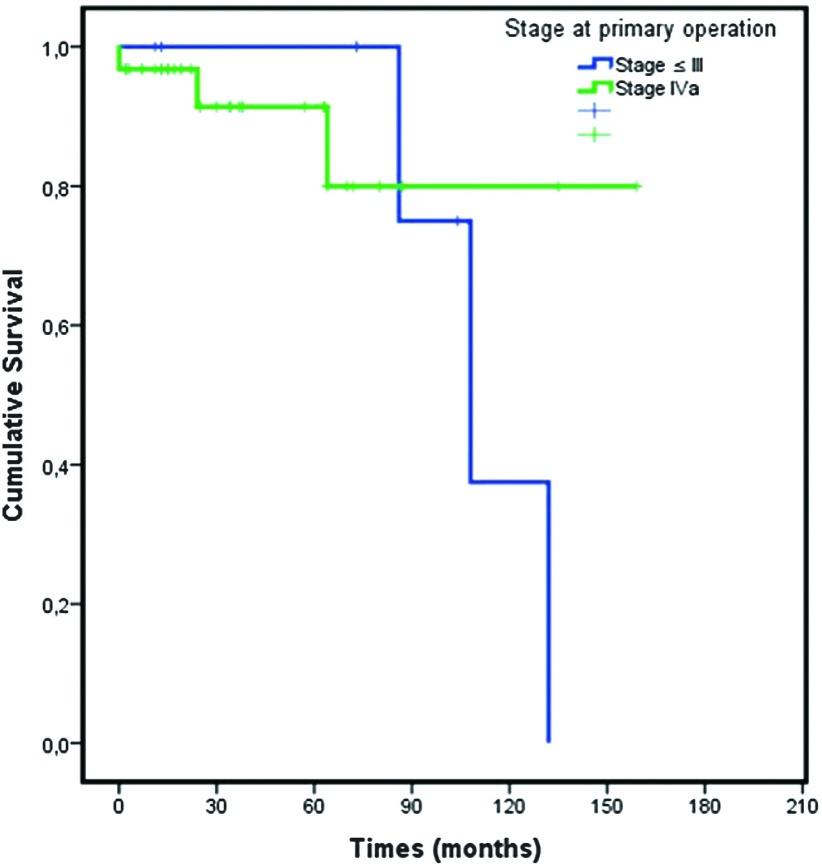
Results: Thymoma B2 was the most common histopathological tumor type (n = 16, 41%). Twenty-six (66.7%) patients underwent primary surgeries for Masaoka stage IVa thymoma, whereas nine (23.1%) underwent secondary surgeries and four (10.3%) underwent tertiary surgeries for pleural or pericardial recurrences. Median survival was 132 ± 25 (82-181; 95% confidence interval [CI]) months. Overall 3-, 5-, and 10-year survival rates were 93%, 93%, and 56%, respectively.
Conclusion: Surgical treatment should be considered as a completion modality to oncological therapy and has the potential to provide long-term survival of Masaoka stage IVa in patients with thymoma. The type of surgery should be determined based on the invasiveness of the lesion.
Keywords: Masaoka stage IVa; surgery; thymoma.
Figures
References
-
- Detterbeck FC, Parsons AM. Thymic tumors. Ann Thorac Surg 2004; 77: 1860-9. - PubMed
-
- Rosai J, Sobin L. Histological classification of tumours of the thymus. In: Rosai J, Sobin L. eds.; World Health Organization International Histological Classification of Tumours. Histological Typing of Tumours of the Thymus; Heidelberg, Springer, 1999; pp 1-16.
-
- Masaoka A, Monden Y, Nakahara K, et al. Follow-up study of thymomas with special reference to their clinical stages. Cancer 1981; 48: 2485-92. - PubMed
-
- Venuta F, Anile M, Diso D, et al. Thymoma and thymic carcinoma. Eur J Cardiothorac Surg 2010; 37: 13-25. - PubMed
-
- Ried M, Guth H, Potzger T, et al. Surgical resection of thymoma still represents the first choice of treatment. Thorac Cardiovasc Surg 2012; 60: 145-9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical