

What do eye movements tell us about patients with neurological disorders? - An introduction to saccade recording in the clinical setting
- PMID: 29225306
- PMCID: PMC5790757
- DOI: 10.2183/pjab.93.049
What do eye movements tell us about patients with neurological disorders? - An introduction to saccade recording in the clinical setting
Abstract
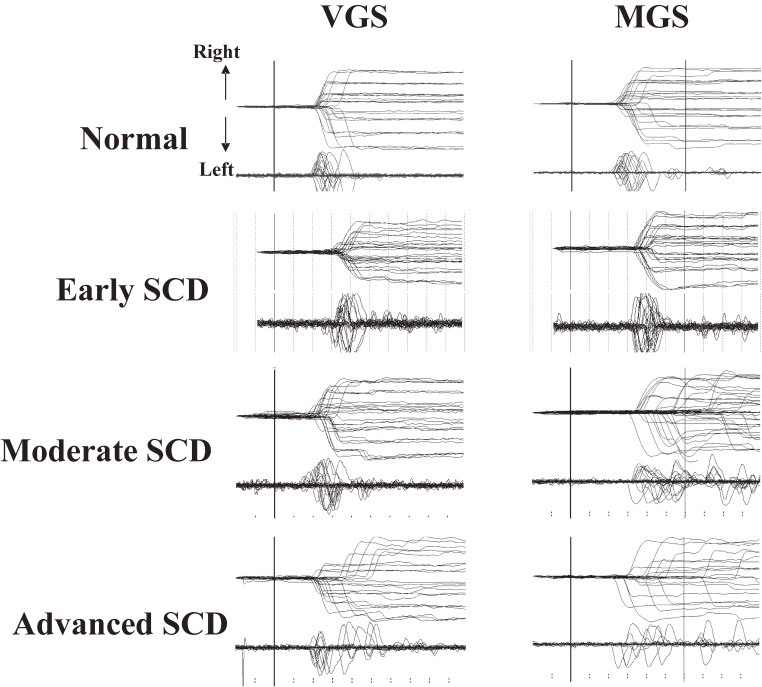
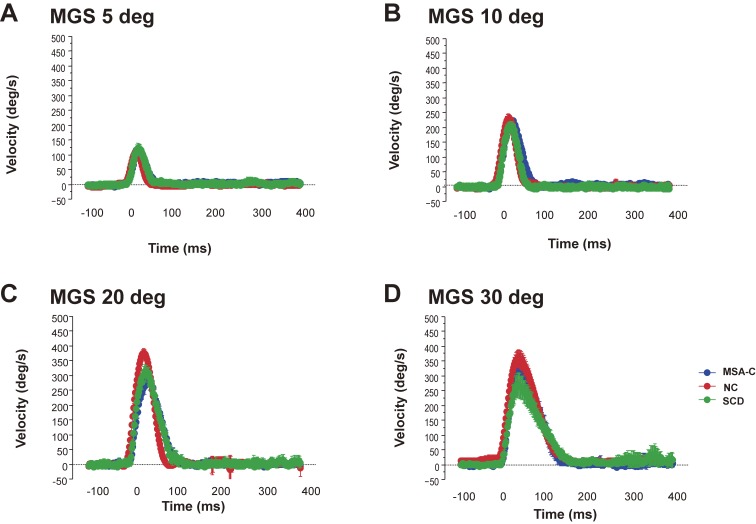
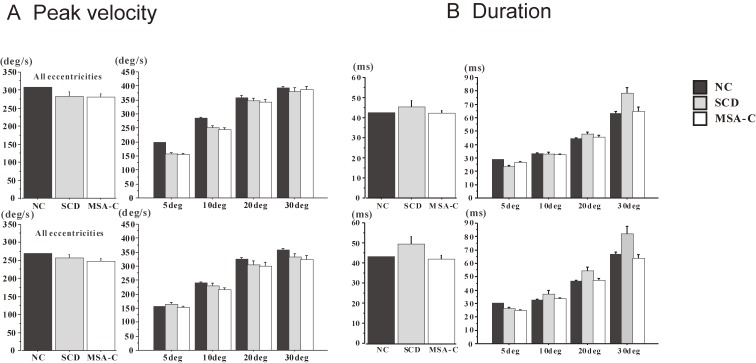
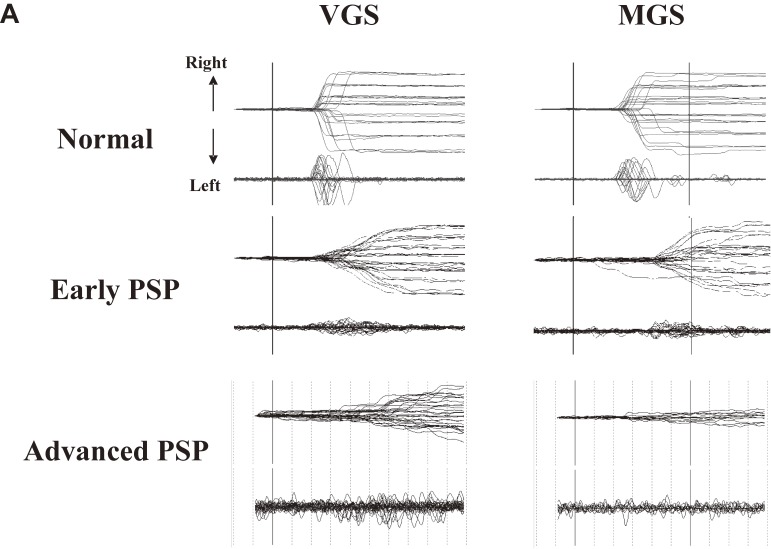
Non-invasive and readily implemented in the clinical setting, eye movement studies have been conducted extensively not only in healthy human subjects but also in patients with neurological disorders. The purpose of saccade studies is to "read out" the pathophysiology underlying neurological disorders from the saccade records, referring to known primate physiology. In the current review, we provide an overview of studies in which we attempted to elucidate the patterns of saccade abnormalities in over 250 patients with neurological disorders, including cerebellar ataxia and brainstem pathology due to neurodegenerative disorders, and what they tell about the pathophysiology of patients with neurological disorders. We also discuss how interventions, such as deep brain stimulation, affect saccade performance and provide further insights into the workings of the oculomotor system in humans. Finally, we argue that it is important to understand the functional significance and behavioral correlate of saccade abnormalities in daily life, which could require eye tracking methodologies to be performed in settings similar to daily life.
Keywords: ataxia; basal ganglia; cerebellum; cerebral cortex; parkinsonism; saccade.
Figures
Similar articles
-
Is multiple system atrophy with cerebellar ataxia (MSA-C) like spinocerebellar ataxia and multiple system atrophy with parkinsonism (MSA-P) like Parkinson's disease? - A saccade study on pathophysiology.Clin Neurophysiol. 2016 Feb;127(2):1491-1502. doi: 10.1016/j.clinph.2015.07.035. Epub 2015 Aug 22. Clin Neurophysiol. 2016. PMID: 26350408
-
Eye movements in patients with neurodegenerative disorders.Nat Rev Neurol. 2013 Feb;9(2):74-85. doi: 10.1038/nrneurol.2012.273. Epub 2013 Jan 22. Nat Rev Neurol. 2013. PMID: 23338283 Review.
-
Differences in saccade dynamics between spinocerebellar ataxia 2 and late-onset cerebellar ataxias.Brain. 2011 Mar;134(Pt 3):879-91. doi: 10.1093/brain/awr009. Brain. 2011. PMID: 21354979
-
[Functional analysis of the thalamocortical pathways in eye movements].Brain Nerve. 2011 Aug;63(8):871-7. Brain Nerve. 2011. PMID: 21817178 Review. Japanese.
-
Positron emission tomography study of voluntary saccadic eye movements and spatial working memory.J Neurophysiol. 1996 Jan;75(1):454-68. doi: 10.1152/jn.1996.75.1.454. J Neurophysiol. 1996. PMID: 8822570
Cited by
-
Eye Movements during Measurements of Visual Vertical in the Poststroke Subacute Phase.eNeuro. 2025 Jan 17;12(1):ENEURO.0279-24.2024. doi: 10.1523/ENEURO.0279-24.2024. Print 2025 Jan. eNeuro. 2025. PMID: 39746806 Free PMC article.
-
Significance of clinical symptoms and red flags in early differential diagnosis of Parkinson's disease and atypical Parkinsonian syndromes.J Neural Transm (Vienna). 2023 Jun;130(6):839-846. doi: 10.1007/s00702-023-02634-5. Epub 2023 Apr 12. J Neural Transm (Vienna). 2023. PMID: 37046147 Free PMC article.
-
Do Miniature Eye Movements Affect Neurofeedback Training Performance? A Combined EEG-Eye Tracking Study.Appl Psychophysiol Biofeedback. 2024 Jun;49(2):313-327. doi: 10.1007/s10484-024-09625-6. Epub 2024 Mar 16. Appl Psychophysiol Biofeedback. 2024. PMID: 38492124 Free PMC article.
-
Eye Movement Disorders in Movement Disorders.Mov Disord Clin Pract. 2022 Feb 16;9(3):284-295. doi: 10.1002/mdc3.13413. eCollection 2022 Apr. Mov Disord Clin Pract. 2022. PMID: 35402641 Free PMC article. Review.
-
Assessing Saccadic Eye Movements With Head-Mounted Display Virtual Reality Technology.Front Psychiatry. 2020 Sep 17;11:572938. doi: 10.3389/fpsyt.2020.572938. eCollection 2020. Front Psychiatry. 2020. PMID: 33093838 Free PMC article.
References
-
- Yarbus, A.L. (1967) Eye Movements and Vision (B. Haigh, Trans.). Plenum Press, New York.
-
- Rayner K. (2009) Eye movements and landing positions in reading: a retrospective. Perception 38, 895–899. - PubMed
-
- Gilchrist I.D., Brown V., Findlay J.M. (1997) Saccades without eye movements. Nature 390, 130–131. - PubMed
-
- Hayhoe M., Ballard D. (2005) Eye movements in natural behavior. Trends Cogn. Sci. 9, 188–194. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical