

Laparoscopic complete mesocolic excisions for colonic cancer in the last decade: Five-year survival in a single centre
- PMID: 29225732
- PMCID: PMC5714803
- DOI: 10.4240/wjgs.v9.i11.215
Laparoscopic complete mesocolic excisions for colonic cancer in the last decade: Five-year survival in a single centre
Abstract
Aim: To analyse clinical and long-term oncologic results after laparoscopic complete mesocolic excision (CME) for colonic cancer over a 10-year period.
Methods: Consecutive patients who received laparoscopic CME at our hospital from 2007 to 2017 were prospectively registered and retrospectively analysed. In total, 341 patients were included with tumour-nodal-metastasis (TNM) stages 0-III.
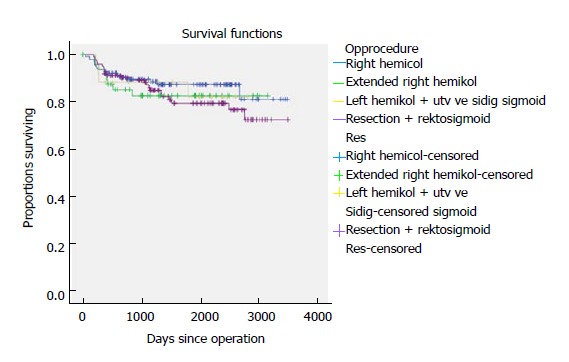
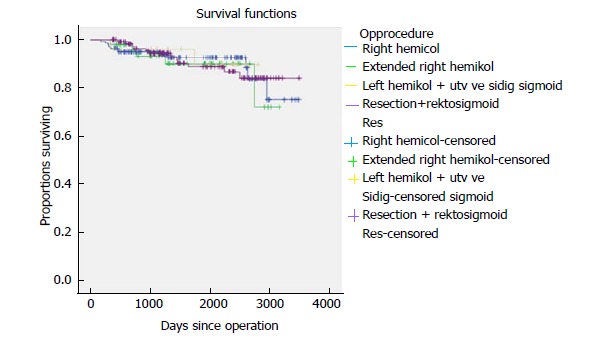
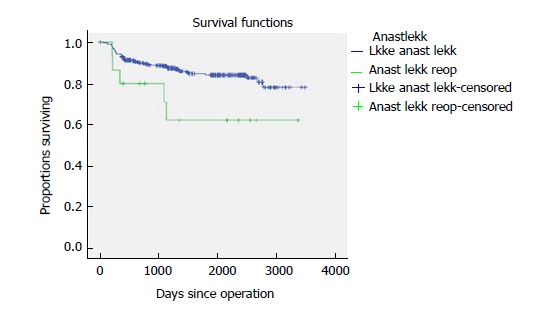
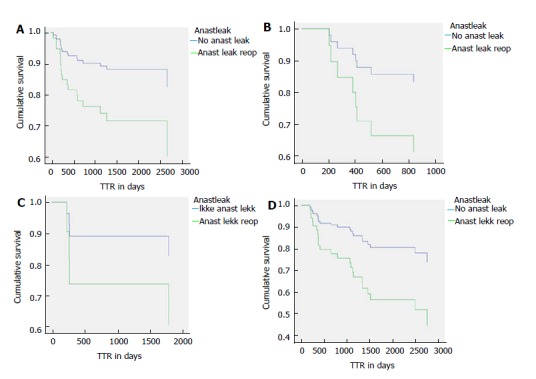
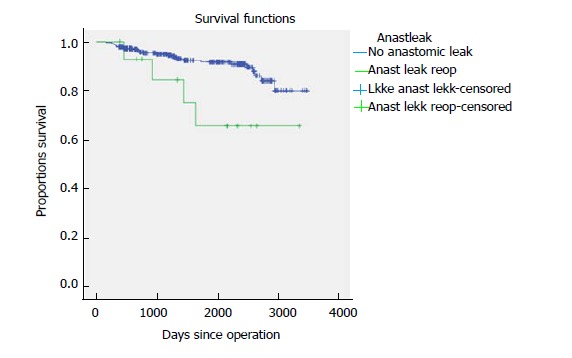
Results: The mean age of the patients was 71.9 years. The median length of stay was 5 d. The mean lymph node harvest was 17.8. The mortality rate was 1.2%. Fifteen patients were reoperated on for anastomotic leaks. The local recurrence rate was 2.3%. Five-year TTR and cancer-specific survival CSS were 83.1% and 90.3%. The location of the tumour was not a significant variable for survival in unadjusted and adjusted survival analysis. TNM stage and anastomotic leaks were significant variables with respect to survival.
Conclusion: Laparoscopic CME results in acceptable complication rates and long-term oncologic results. It is important to avoid anastomotic leaks because of their negative effect on survival.
Keywords: Cancer specific survival; Central vascular ligature; Colonic cancer; Complete mesocolic excision; Laparoscopic surgery; Time to recurrence.
Conflict of interest statement
Conflict-of-interest statement: The authors of this manuscript have no conflict- of- interest to disclose.
Figures
References
-
- Hohenberger W, Reingruber B, Merkel S. Surgery for colon cancer. Scand J Surg. 2003;92:45–52. - PubMed
-
- Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation--technical notes and outcome. Colorectal Dis. 2009;11:354–364; discussion 364-365. - PubMed
-
- Yamamoto S, Inomata M, Katayama H, Mizusawa J, Etoh T, Konishi F, Sugihara K, Watanabe M, Moriya Y, Kitano S; Japan Clinical Oncology Group Colorectal Cancer Study Group. Short-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer: Japan Clinical Oncology Group Study JCOG 0404. Ann Surg. 2014;260:23–30. - PubMed
-
- West NP, Kobayashi H, Takahashi K, Perrakis A, Weber K, Hohenberger W, Sugihara K, Quirke P. Understanding optimal colonic cancer surgery: comparison of Japanese D3 resection and European complete mesocolic excision with central vascular ligation. J Clin Oncol. 2012;30:1763–1769. - PubMed
-
- Søndenaa K, Quirke P, Hohenberger W, Sugihara K, Kobayashi H, Kessler H, Brown G, Tudyka V, D’Hoore A, Kennedy RH, et al. The rationale behind complete mesocolic excision (CME) and a central vascular ligation for colon cancer in open and laparoscopic surgery: proceedings of a consensus conference. Int J Colorectal Dis. 2014;29:419–428. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
