

Seasonal clustering of sinopulmonary mucormycosis in patients with hematologic malignancies at a large comprehensive cancer center
- PMID: 29225797
- PMCID: PMC5718160
- DOI: 10.1186/s13756-017-0282-0
Seasonal clustering of sinopulmonary mucormycosis in patients with hematologic malignancies at a large comprehensive cancer center
Abstract
Background: Invasive Mucorales infections (IMI) lead to significant morbidity and mortality in immunocompromised hosts. The role of season and climatic conditions in case clustering of IMI remain poorly understood.
Methods: Following detection of a cluster of sinopulmonary IMIs in patients with hematologic malignancies, we reviewed center-based medical records of all patients with IMIs and other invasive fungal infections (IFIs) between January of 2012 and August of 2015 to assess for case clustering in relation to seasonality.
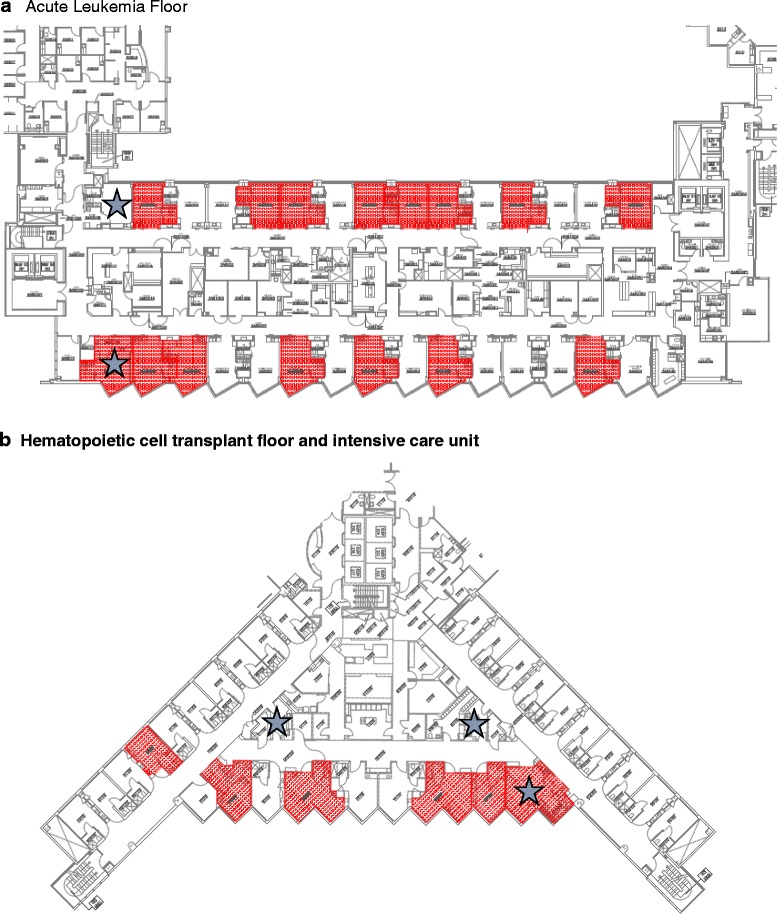
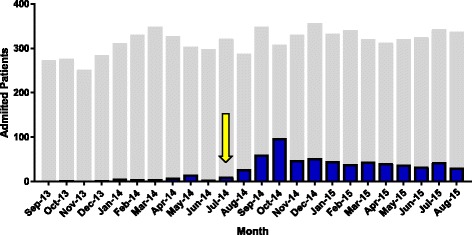
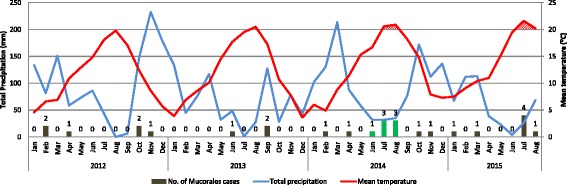
Results: A cluster of 7 patients were identified with sinopulmonary IMIs (Rhizopus microsporus/azygosporus, 6; Rhizomucor pusillus, 1) during a 3 month period between June and August of 2014. All patients died or were discharged to hospice. The cluster was managed with institution of standardized posaconazole prophylaxis to high-risk patients and patient use of N-95 masks when outside of protected areas on the inpatient service. Review of an earlier study period identified 11 patients with IMIs of varying species over the preceding 29 months without evidence of clustering. There were 9 total IMIs in the later study period (12 month post-initial cluster) with 5 additional cases in the summer months, again suggesting seasonal clustering. Extensive environmental sampling did not reveal a source of mold. Using local climatological data abstracted from National Centers for Environmental Information the clusters appeared to be associated with high temperatures and low precipitation.
Conclusions: Sinopulmonary Mucorales clusters at our center had a seasonal variation which appeared to be related to temperature and precipitation. Given the significant mortality associated with IMIs, local climatic conditions may need to be considered when considering center specific fungal prevention and prophylaxis strategies for high-risk patients.
Keywords: Climate; Fungus; Healthcare-associated infections; Immunocompromised host; Mold; Mucormycosis; Seasonal.
Conflict of interest statement
Ethics approval and consent to participate
Fred Hutchinson Cancer Research Center Institution Review Board provided ethics approval for the conduct of this study.
Consent for publication
Not applicable
Competing interests
Data from this manuscript have been presented in part at the IDWeek in San Diego, CA October 2015. SAP has received research support from Chimerix, Merck, and has been a consultant from Merck and Optimer/Cubist Pharmaceuticals.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
