

Neuroanatomy and Neuropsychology of Pain
- PMID: 29226044
- PMCID: PMC5718877
- DOI: 10.7759/cureus.1754
Neuroanatomy and Neuropsychology of Pain
Abstract
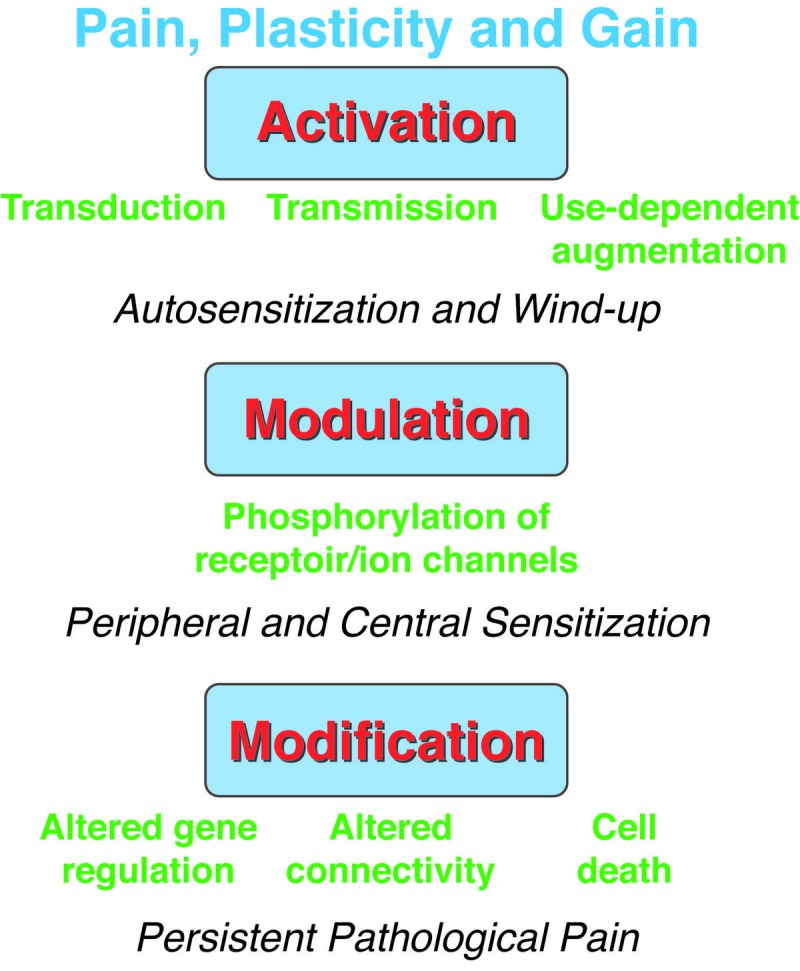
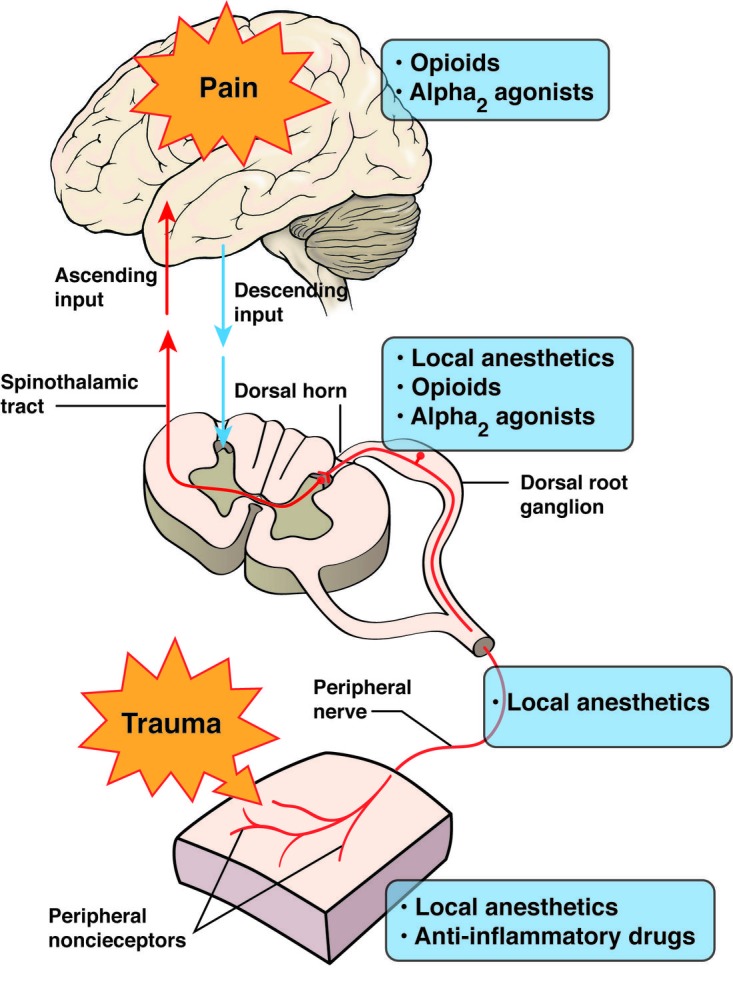
We have reviewed here the neuroanatomical and neuropsychological literature of the human brain and have proposed the various pain mechanisms that we currently know of. Essentially when tissue is damaged, peripheral nociceptors are activated continuously and prostanoids are hence produced. Nonsteroidal anti-inflammatory drugs (NSAIDs) and medications aim to target these prostanoids to treat the inflammatory component of pain. Normal pain tends to have a protective response. It is important for the nervous system to learn and recognize this painful stimulus earlier and quicker with repeated exposure to avoid tissue damage. This neuronal plasticity and gain in sensitivity result in sensitization of the nervous system, both centrally and peripherally and help in earlier detection of the pain sensation. However, persistent pain can become pathologic and will eventually result in the loss of protection pain offers to the body. Pain-related fear has been implicated in the transition from acute to chronic low back pain and the persistence of disabling low back pain, making it a key target for physiotherapy intervention. The current understanding of pain-related fear is that it is a psychopathological problem where people who catastrophise about the meaning of pain become trapped in a vicious cycle of avoidance behaviour, pain and disability, as recognised in the fear-avoidance model. We looked at how pain is perceived, especially in low-back pain patients. It has been hypothesized that individuals with low-back pain (LBP) can change their motor behavior, which is fundamentally an adaptation mechanism aimed at minimizing the real or perceived risk of further pain.
Keywords: motor control; neuroanatomy; neuropsychology; nociception; orbitofrontal cortex; pain; reinforcement learning.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Making Sense of Low Back Pain and Pain-Related Fear.J Orthop Sports Phys Ther. 2017 Sep;47(9):628-636. doi: 10.2519/jospt.2017.7434. Epub 2017 Jul 13. J Orthop Sports Phys Ther. 2017. PMID: 28704621
-
[Pathophysiology of low back pain and the transition to the chronic state - experimental data and new concepts].Schmerz. 2001 Dec;15(6):413-7. doi: 10.1007/s004820100002. Schmerz. 2001. PMID: 11793144 German.
-
The functional neuroanatomy of the human orbitofrontal cortex: evidence from neuroimaging and neuropsychology.Prog Neurobiol. 2004 Apr;72(5):341-72. doi: 10.1016/j.pneurobio.2004.03.006. Prog Neurobiol. 2004. PMID: 15157726 Review.
-
Pathogenesis of Pain.Semin Pediatr Neurol. 2016 Aug;23(3):201-208. doi: 10.1016/j.spen.2016.10.003. Epub 2016 Oct 14. Semin Pediatr Neurol. 2016. PMID: 27989327 Review.
-
Fear-avoidance beliefs, disability, and participation in workers and non-workers with acute low back pain.Clin J Pain. 2006 Jan;22(1):45-54. doi: 10.1097/01.ajp.0000148626.84874.93. Clin J Pain. 2006. PMID: 16340593
Cited by
-
Spinal pain in employees exposed to abusive supervision: Evidence of a sex and CRHR1 CTC haplotype interaction.Mol Pain. 2021 Jan-Dec;17:17448069211042123. doi: 10.1177/17448069211042123. Mol Pain. 2021. PMID: 34617831 Free PMC article.
-
The Delta-Opioid Receptor; a Target for the Treatment of Pain.Front Mol Neurosci. 2020 May 5;13:52. doi: 10.3389/fnmol.2020.00052. eCollection 2020. Front Mol Neurosci. 2020. PMID: 32431594 Free PMC article. Review.
-
Analgesia for the Bayesian Brain: How Predictive Coding Offers Insights Into the Subjectivity of Pain.Curr Pain Headache Rep. 2023 Nov;27(11):631-638. doi: 10.1007/s11916-023-01122-5. Epub 2023 Jul 8. Curr Pain Headache Rep. 2023. PMID: 37421540 Free PMC article. Review.
-
Deciphering distinct spatial alterations in N-glycan expression profiles in the spinal cord and brain of male rats in a neuropathic pain model.Cell Mol Biol Lett. 2025 Mar 11;30(1):31. doi: 10.1186/s11658-025-00709-7. Cell Mol Biol Lett. 2025. PMID: 40069587 Free PMC article.
-
Brainstem Diffusion Tensor Tractography and Clinical Applications in Pain.Front Pain Res (Lausanne). 2022 Mar 24;3:840328. doi: 10.3389/fpain.2022.840328. eCollection 2022. Front Pain Res (Lausanne). 2022. PMID: 35399154 Free PMC article. Review.
References
-
- Pathogenesis of pain. Dinakar P, Stillman AM. Semin Pediatr Neurol. 2016;23:201–208. - PubMed
-
- Relieving pain in America: insights from an Institute of Medicine Committee. Dzau VJ, Pizzo PA. J Am Med Assoc. 2014;312:1507–1508. - PubMed
-
- Lost productive time and cost due to common pain conditions in the US workforce. Stewart WF, Ricci JA, Chee E. J Am Med Assoc. 2003;290:2443–2454. - PubMed
-
- The economic costs of pain in the United States. Gaskin DJ, Richard P. J Pain. 2012;13:715–724. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous