

Towards personalized, tumour-specific, therapeutic vaccines for cancer
- PMID: 29226910
- PMCID: PMC6508552
- DOI: 10.1038/nri.2017.131
Towards personalized, tumour-specific, therapeutic vaccines for cancer
Abstract
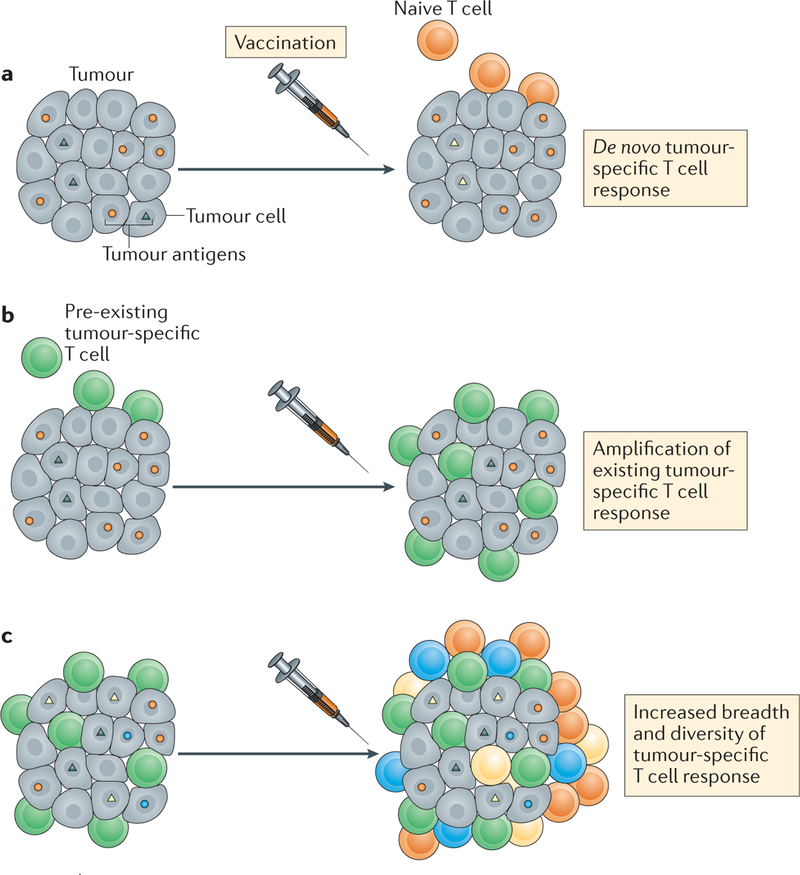
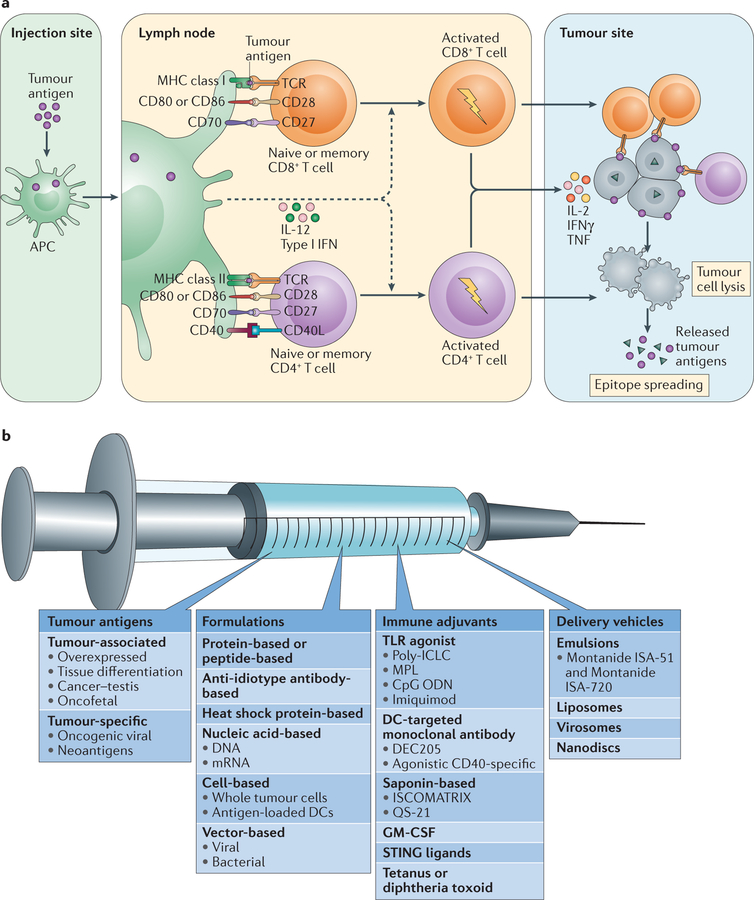
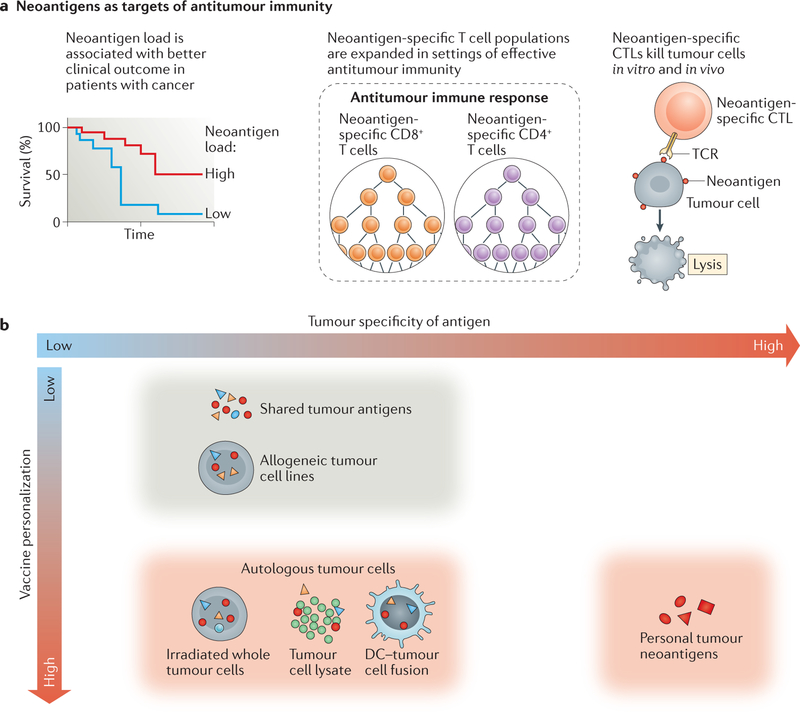
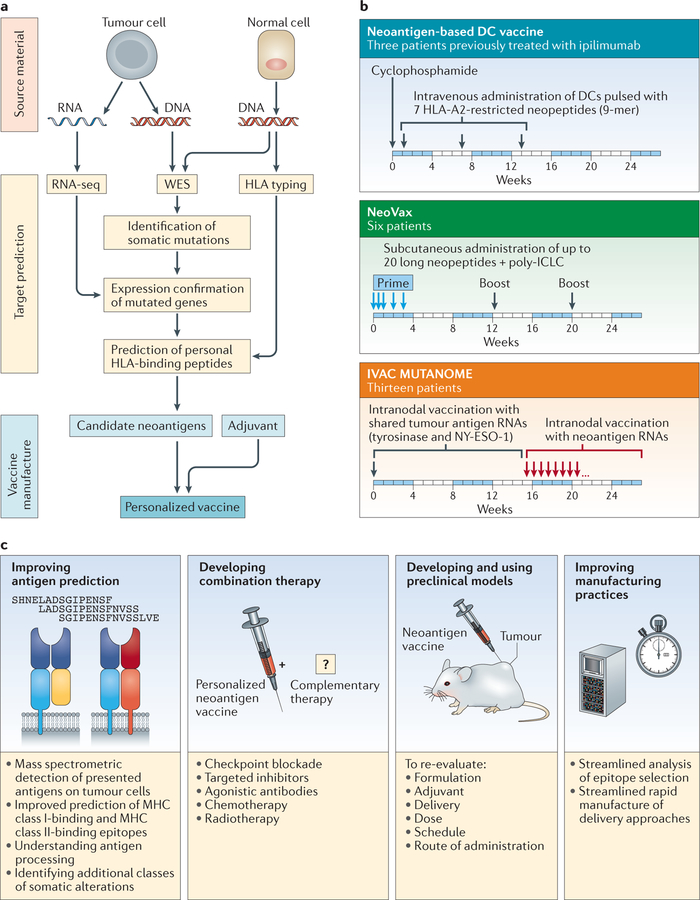
Cancer vaccines, which are designed to amplify tumour-specific T cell responses through active immunization, have long been envisioned as a key tool of effective cancer immunotherapy. Despite a clear rationale for such vaccines, extensive past efforts were unsuccessful in mediating clinically relevant antitumour activity in humans. Recently, however, next-generation sequencing and novel bioinformatics tools have enabled the systematic discovery of tumour neoantigens, which are highly desirable immunogens because they arise from somatic mutations of the tumour and are therefore tumour specific. As a result of the diversity of tumour neoepitopes between individuals, the development of personalized cancer vaccines is warranted. Here, we review the emerging field of personalized cancer vaccination and discuss recent developments and future directions for this promising treatment strategy.
Conflict of interest statement
Competing interests statement
The authors declare competing interests; see Web version for details.
Figures
References
-
- Coulie PG, Van den Eynde BJ, van der Bruggen P & Boon T Tumour antigens recognized by T lymphocytes: at the core of cancer immunotherapy. Nat. Rev. Cancer 14, 135–146 (2014). - PubMed
-
- Wong KK, Li WA, Mooney DJ & Dranoff G Advances in therapeutic cancer vaccines. Adv. Immunol 130, 191–249 (2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
