

Practice Patterns and Outcomes Associated With Early Sedation Depth in Mechanically Ventilated Patients: A Systematic Review and Meta-Analysis
- PMID: 29227367
- PMCID: PMC5825247
- DOI: 10.1097/CCM.0000000000002885
Practice Patterns and Outcomes Associated With Early Sedation Depth in Mechanically Ventilated Patients: A Systematic Review and Meta-Analysis
Abstract
Objectives: Emerging data suggest that early deep sedation may negatively impact clinical outcomes. This systematic review and meta-analysis defines and quantifies the impact of deep sedation within 48 hours of initiation of mechanical ventilation, as described in the world's literature. The primary outcome was mortality. Secondary outcomes included hospital and ICU lengths of stay, mechanical ventilation duration, and delirium and tracheostomy frequency.
Data sources: The following data sources were searched: MEDLINE, EMBASE, Scopus, Cochrane Central Register of Controlled Trials, Database of Abstracts of Reviews and Effects, Cochrane Database of Systematic Reviews databases, ClinicalTrials.gov, conference proceedings, and reference lists.
Study selection: Randomized controlled trials and nonrandomized studies were included.
Data extraction: Two reviewers independently screened abstracts of identified studies for eligibility.
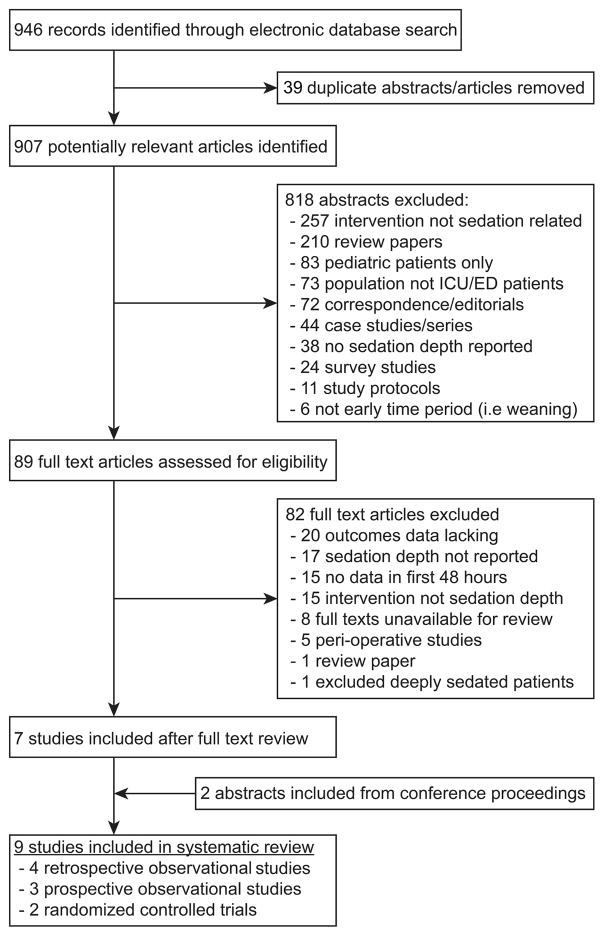
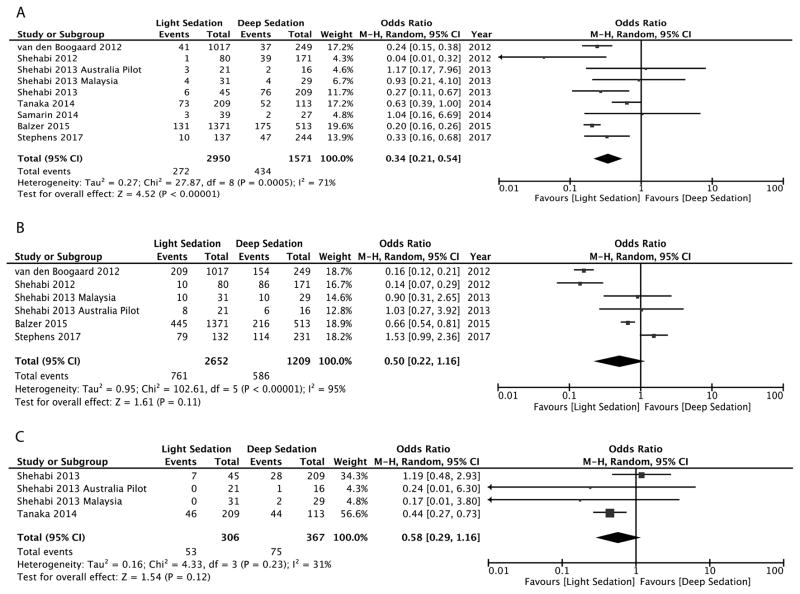
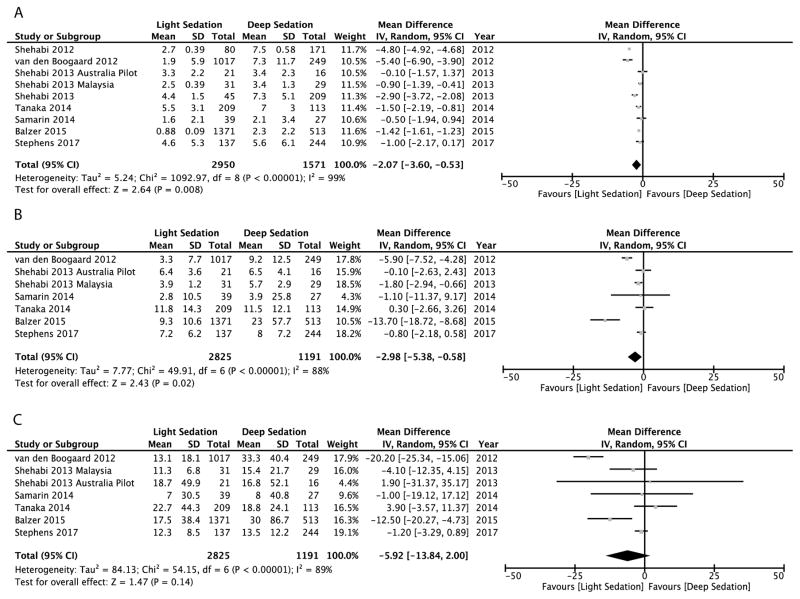
Data synthesis: Nine studies (n = 4,521 patients) published between 2012 and 2017 were included. A random effects meta-analytic model revealed that early light sedation was associated with lower mortality (9.2%) versus deep sedation (27.6%) (odds ratio, 0.34 [0.21-0.54]). Light sedation was associated with fewer mechanical ventilation (mean difference, -2.1; 95% CI, -3.6 to -0.5) and ICU days (mean difference, -3.0 (95% CI, -5.4 to -0.6). Delirium frequency was 28.7% in the light sedation group and 48.5% in the deep sedation group, odds ratio, 0.50 (0.22-1.16).
Conclusions: Deep sedation in mechanically ventilated patients, as evaluated in a small number of qualifying heterogeneous randomized controlled trials and observational studies, was associated with increased mortality and lengths of stay. Interventions targeting early sedation depth assessment, starting in the emergency department and subsequent ICU admission, deserve further investigation and could improve outcome.
Conflict of interest statement
Figures
Comment in
-
The Golden Hours of ICU Sedation: The Clock Is Ticking..Crit Care Med. 2018 Mar;46(3):490-491. doi: 10.1097/CCM.0000000000002902. Crit Care Med. 2018. PMID: 29474335 No abstract available.
References
-
- Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. - PubMed
-
- Shehabi Y, Bellomo R, Reade MC, et al. Early goal-directed sedation versus standard sedation in mechanically ventilated critically ill patients: a pilot study*. Crit Care Med. 2013;41(8):1983–1991. - PubMed
-
- Shehabi Y, Bellomo R, Reade MC, et al. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am J Respir Crit Care Med. 2012;186:724–731. - PubMed
-
- Foy R. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann Intern Med. 2010;151:264–269. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
