

Antibiotic Resistance and the Risk of Recurrent Bacteremia
- PMID: 29228127
- PMCID: PMC5960995
- DOI: 10.1093/cid/cix1076
Antibiotic Resistance and the Risk of Recurrent Bacteremia
Abstract
Background: Direct health effects of antibiotic resistance are difficult to assess. We quantified the risk of recurrent bacteremia associated with resistance.
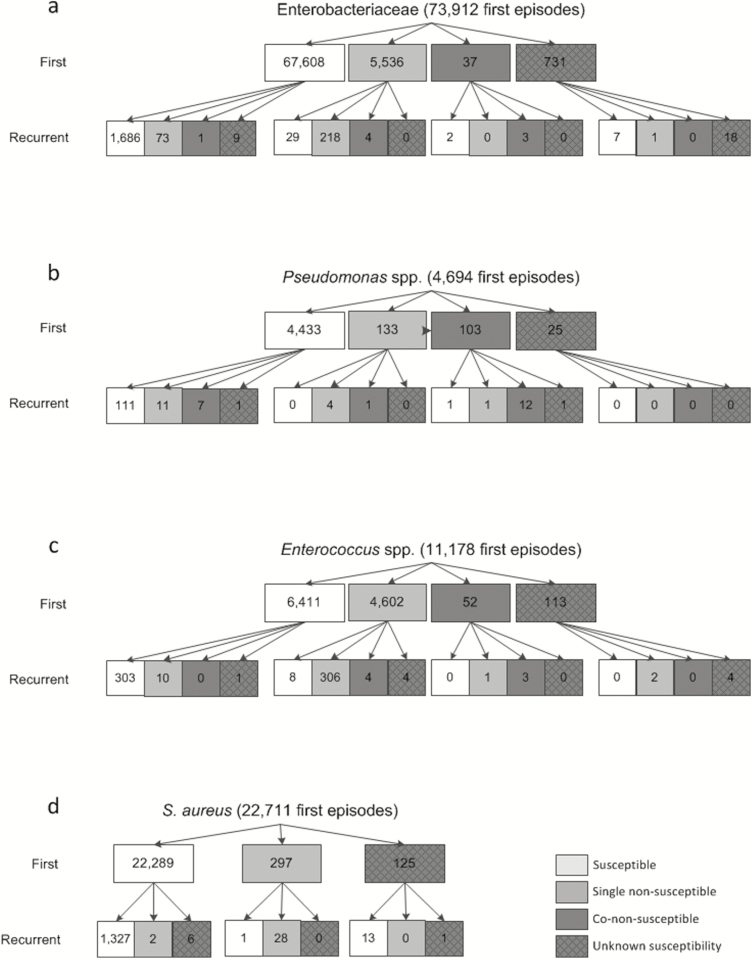
Methods: We extracted antimicrobial susceptibility testing data on blood isolates from the Dutch surveillance system for antimicrobial resistance between 2008 and 2017. First and first recurrent (4-30 days) bacteremia episodes were categorized as susceptible, single nonsusceptible, or co-nonsusceptible to third-generation cephalosporins without or with carbapenems (Enterobacteriaceae), ceftazidime without or with carbapenems (Pseudomonas species), aminopenicillins without or with vancomycin (Enterococcus species), or as methicillin-sensitive/-resistant S. aureus (MSSA/MRSA). We calculated risks of recurrent bacteremia after nonsusceptible vs susceptible first bacteremia, estimated the crude population attributable effect of resistance for the Netherlands, and calculated risks of nonsusceptible recurrent bacteremia after a susceptible first episode.
Results: Risk ratios for recurrent bacteremia after a single- and co-nonsusceptible first episode, respectively, vs susceptible first episode, were 1.7 (95% confidence interval [CI], 1.5-2.0) and 5.2 (95% CI, 2.1-12.4) for Enterobacteriaceae, 1.3 (95% CI, 0.5-3.1) and 5.0 (95% CI, 2.9-8.5) for Pseudomonas species, 1.4 (95% CI, 1.2-1.7) and 1.6 (95% CI, 0.6-4.2) for Enterococcus species, and 1.6 (95% CI, 1.1-2.4) for MRSA vs MSSA. The estimated population annual number of recurrent bacteremias associated with nonsusceptibility was 40. The risk of nonsusceptible recurrent bacteremia after a susceptible first episode was at most 0.4% (Pseudomonas species).
Conclusions: Although antibiotic nonsusceptibility was consistently associated with higher risks of recurrent bacteremia, the estimated annual number of additional recurrent episodes in the Netherlands (40) was rather limited.
Figures
References
-
- Dautzenberg MJ, Wekesa AN, Gniadkowski M, et al. . Mastering Hospital Antimicrobial Resistance in Europe Work Package 3 Study Team The association between colonization with carbapenemase-producing Enterobacteriaceae and overall ICU mortality: an observational cohort study. Crit Care Med 2015; 43:1170–7. - PMC - PubMed
-
- Stewardson AJ, Allignol A, Beyersmann J, et al. . The health and economic burden of bloodstream infections caused by antimicrobial-susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: a multicentre retrospective cohort study. Euro Surveill 2016; 21. doi:10.2807/1560-7917.ES.2016.21.33.30319. - PMC - PubMed
-
- de Kraker ME, Wolkewitz M, Davey PG, et al. . Burden of antimicrobial resistance in European hospitals: excess mortality and length of hospital stay associated with bloodstream infections due to Escherichia coli resistant to third-generation cephalosporins. J Antimicrob Chemother 2011; 66:398–407. - PubMed
-
- Wolkewitz M, Cooper BS, Bonten MJ, Barnett AG, Schumacher M. Interpreting and comparing risks in the presence of competing events. BMJ 2014; 349:g5060. - PubMed
-
- Rottier WC, Ammerlaan HS, Bonten MJ. Effects of confounders and intermediates on the association of bacteraemia caused by extended-spectrum β-lactamase-producing Enterobacteriaceae and patient outcome: a meta-analysis. J Antimicrob Chemother 2012; 67:1311–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
