

Widespread brain tau and its association with ageing, Braak stage and Alzheimer's dementia
- PMID: 29228201
- PMCID: PMC5837250
- DOI: 10.1093/brain/awx320
Widespread brain tau and its association with ageing, Braak stage and Alzheimer's dementia
Abstract
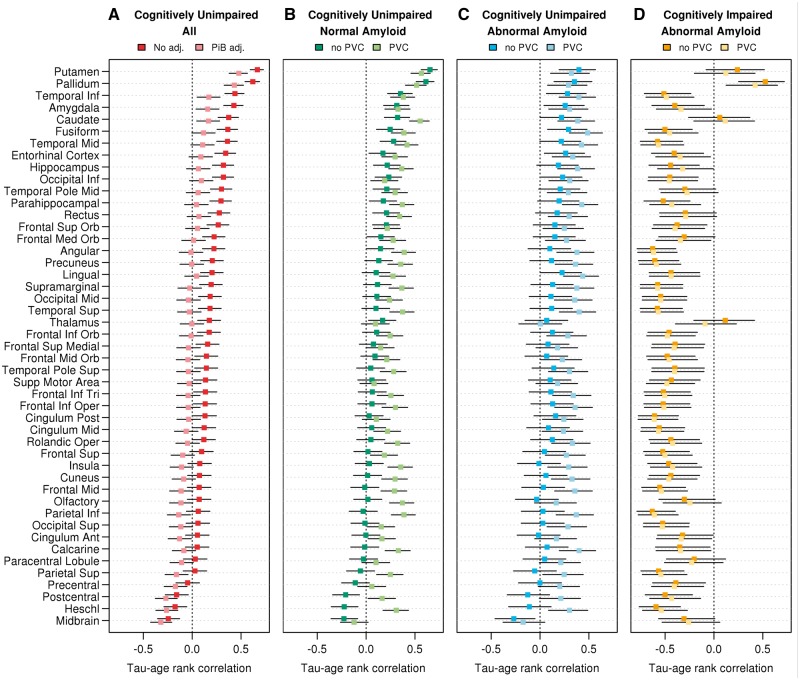
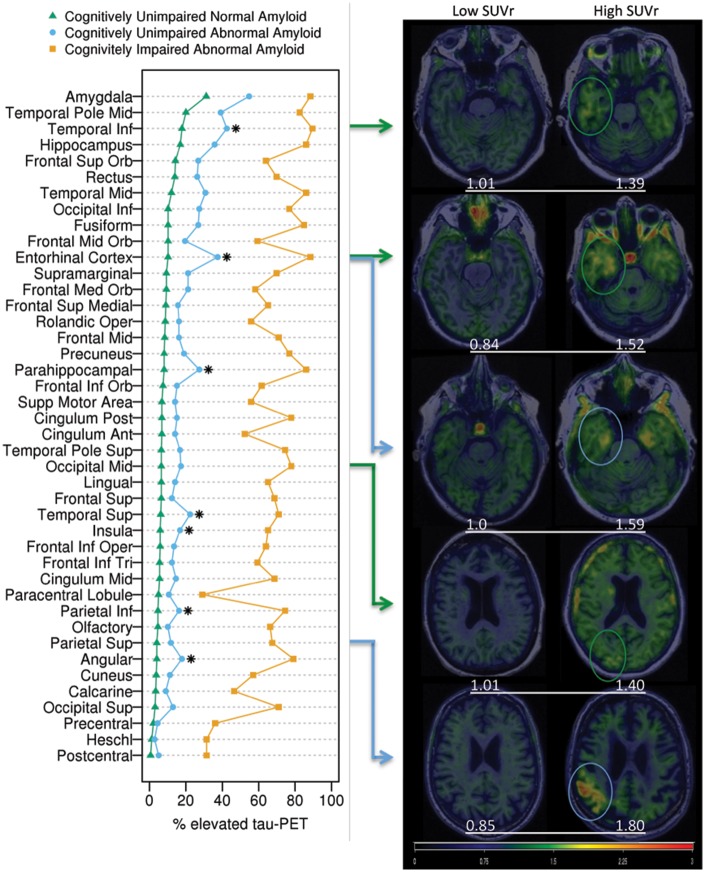
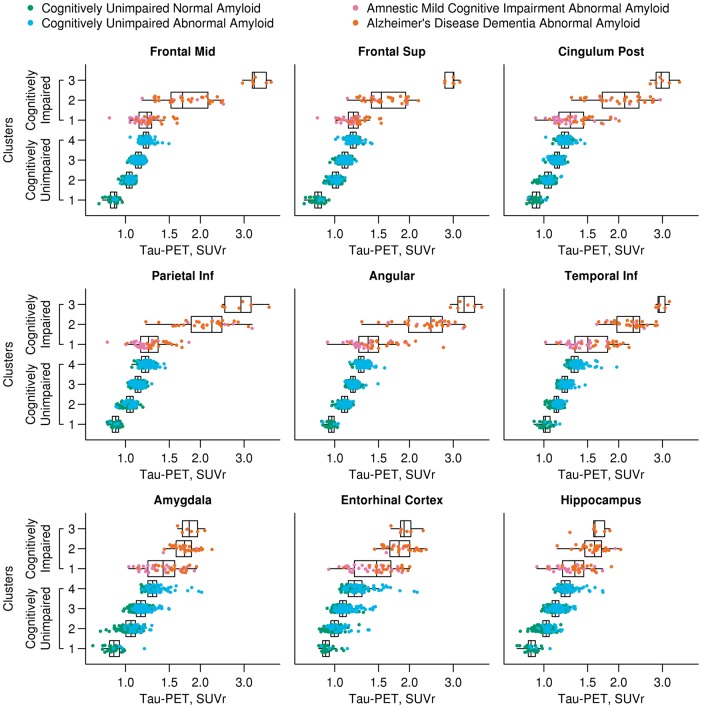
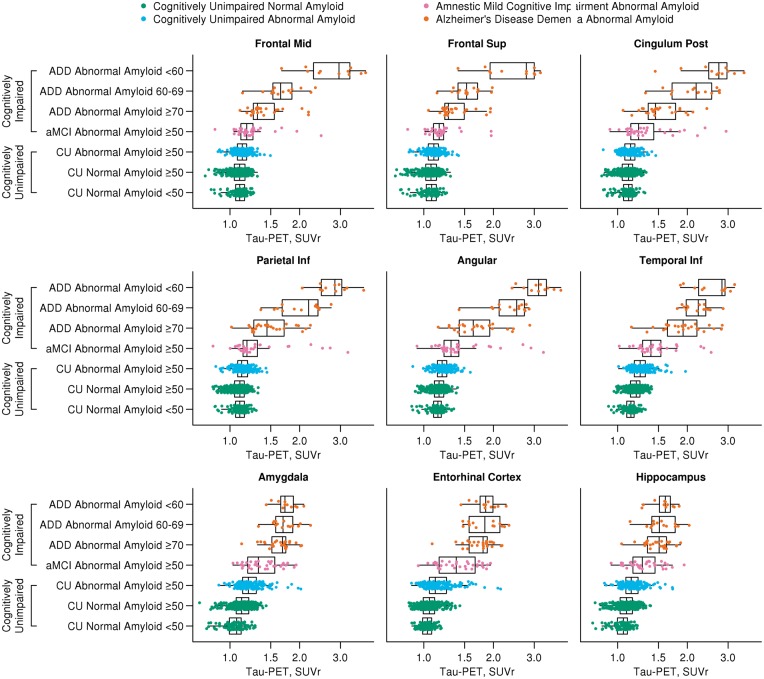
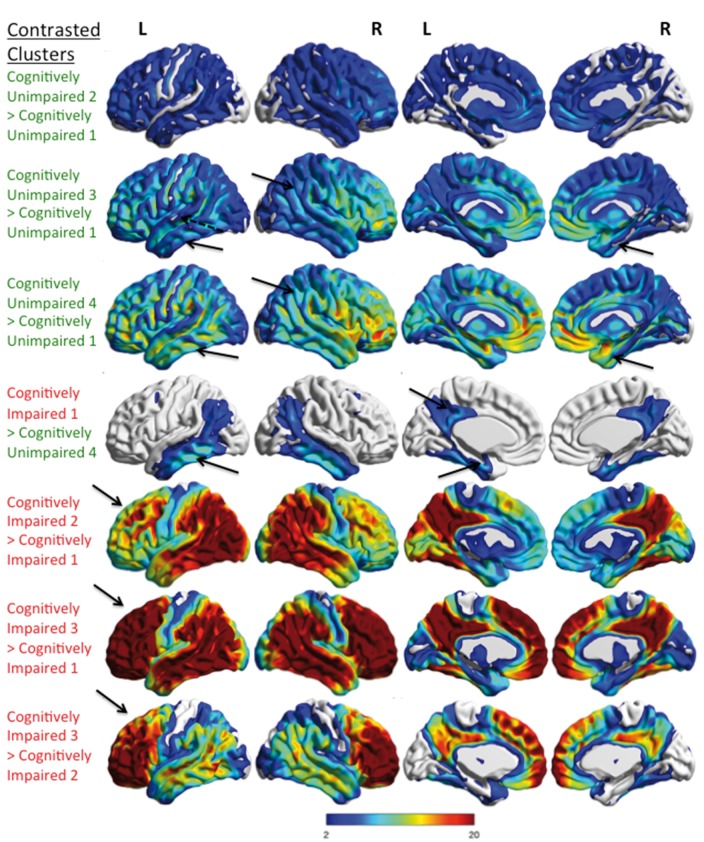
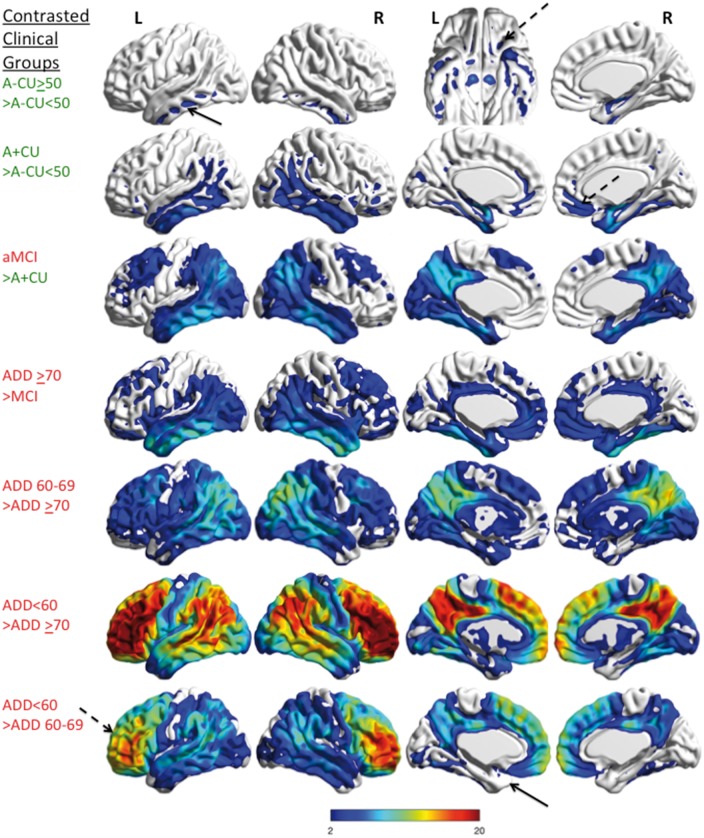
See Herholz (doi:10.1093/brain/awx340) for a scientific commentary on this article.Autopsy data have proposed that a topographical pattern of tauopathy occurs in the brain with the development of dementia due to Alzheimer's disease. We evaluated the findings of tau-PET to better understand neurofibrillary tangle development as it is seen in cognitively unimpaired and impaired individuals. The evolution of Alzheimer's disease tauopathy in cognitively unimpaired individuals needs to be examined to better understand disease pathogenesis. Tau-PET was performed in 86 cognitively impaired individuals who all had abnormal amyloid levels and 601 cognitively unimpaired individuals. Tau-PET findings were assessed for relationships with clinical diagnosis, age, and regional uptake patterns relative to Braak stage. Regional and voxel-wise analyses were performed. Topographical findings from tau-PET were characterized using hierarchical clustering and clinical characteristic-based subcategorization. In older cognitively unimpaired individuals (≥50 years), widespread, age-related elevated tau signal was seen among those with normal or abnormal amyloid status as compared to younger cognitively unimpaired individuals (30-49 years). More frequent regional tau signal elevation throughout the brain was seen in cognitively unimpaired individuals with abnormal versus normal amyloid. Elevated tau signal was seen in regions that are considered high Braak Stage in cognitively unimpaired and cognitively impaired individuals. Hierarchical clustering and clinical characteristic-based categorizations both showed different patterns of tau signal between groups such as greater tau signal in frontal regions in younger onset Alzheimer's disease dementia participants (most of whom had a dysexecutive clinical presentation). Tau-PET signal increases modestly with age throughout the brain in cognitively unimpaired individuals and elevated tau is seen more often when amyloid brain accumulation is present. Tau signal patterns in cognitively unimpaired correspond to early Braak stage but also suggest tangle involvement in extra-medial temporal and extra-temporal regions that are considered more advanced in the Braak scheme even when amyloid negative. Our findings also suggest the possibility of widespread development of early tangle pathology rather than a pattern defined exclusively by adjacent, region-to-region spread, prior to onset of clinical symptoms. Distinct patterns of neurofibrillary tangle deposition in younger-onset Alzheimer's disease dementia versus older-onset Alzheimer's disease dementia provide evidence for variability in regional tangle deposition patterns and demonstrate that different disease phenotypes have different patterns of tauopathy. Pathological correlation with imaging is needed to assess the implications of these observations.
Keywords: Alzheimer’s disease; amyloid-PET; dementia; mild cognitive impairment; tau-PET.
© The Author (2017). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Spread of tau deposits: can we trust in vivo findings?Brain. 2018 Jan 1;141(1):10-12. doi: 10.1093/brain/awx340. Brain. 2018. PMID: 29325049 No abstract available.
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th edn., text revision Washington, DC: American Psychiatric Association; 2000.
-
- Arriagada PV, Marzloff K, Hyman BT. Distribution of Alzheimer-type pathologic changes in nondemented elderly individuals matches the pattern in Alzheimer's disease. Neurology 1992; 42: 1681–8. - PubMed
-
- Ashburner J, Friston KJ. Unified segmentation. Neuroimage 2005; 26: 839–51. - PubMed
-
- Bennett DA, Schneider JA, Wilson RS, Bienias JL, Arnold SE. Neurofibrillary tangles mediate the association of amyloid load with clinical Alzheimer disease and level of cognitive function. Arch Neurol 2004; 61: 378–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
