

The Magnitude and Time Course of IOP Change in Response to Body Position Change in Nonhuman Primates Measured Using Continuous IOP Telemetry
- PMID: 29228251
- PMCID: PMC5724553
- DOI: 10.1167/iovs.17-22858
The Magnitude and Time Course of IOP Change in Response to Body Position Change in Nonhuman Primates Measured Using Continuous IOP Telemetry
Abstract
Purpose: To study the effect and time course of body position changes on IOP in nonhuman primates.
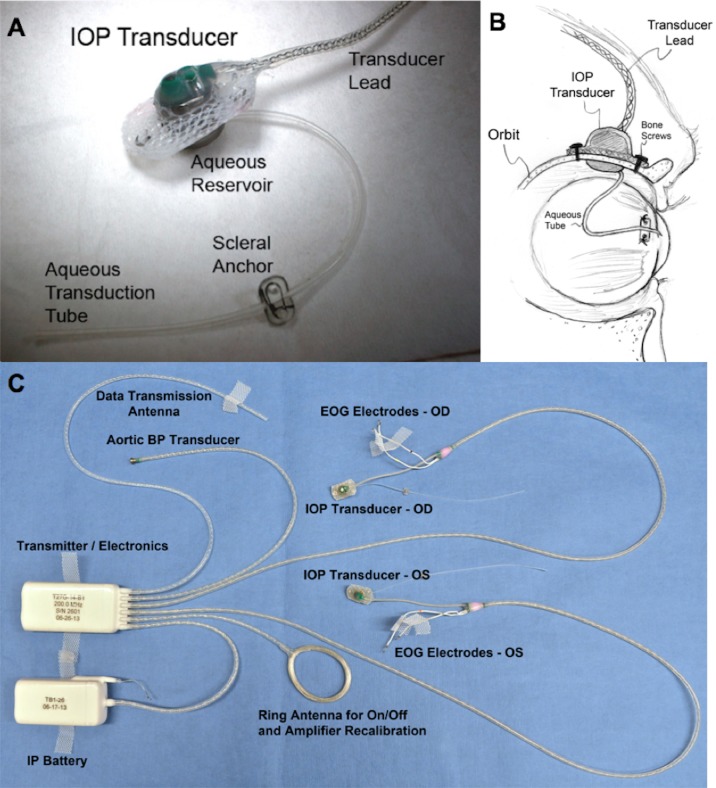
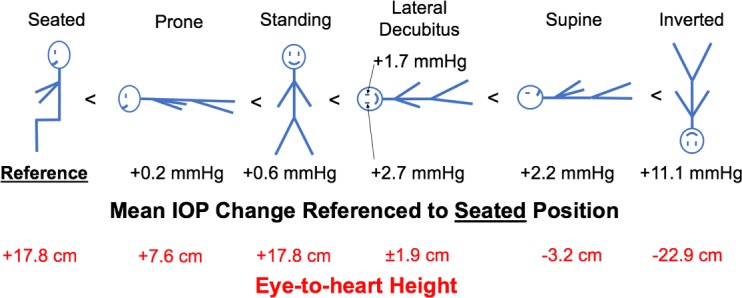
Methods: We recorded continuous bilateral IOP measurements with a wireless telemetry implant in three rhesus macaques in seven different body positions. IOP measurements were acquired in the seated-upright, standing, prone, supine, right and left lateral decubitus positions (LDPs), and head-down inverted positions. Continuous IOP was recorded for 90 seconds in each position before returning to a supine reference position until IOP stabilized; measurements were averaged after IOP stabilized at each position.
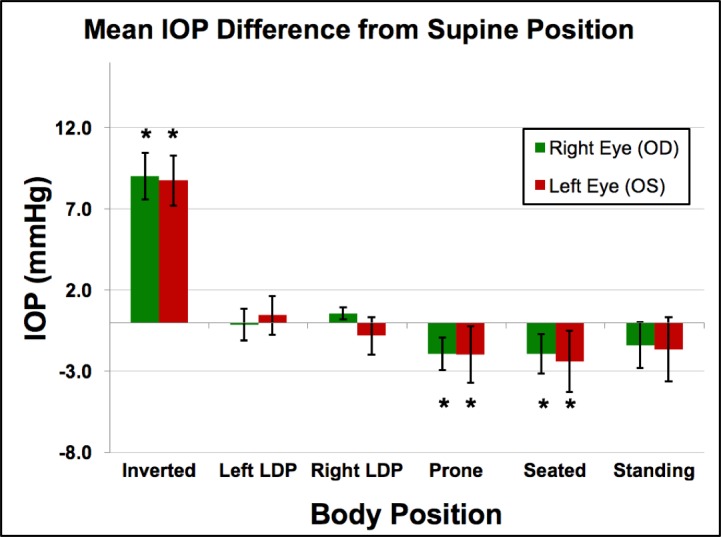
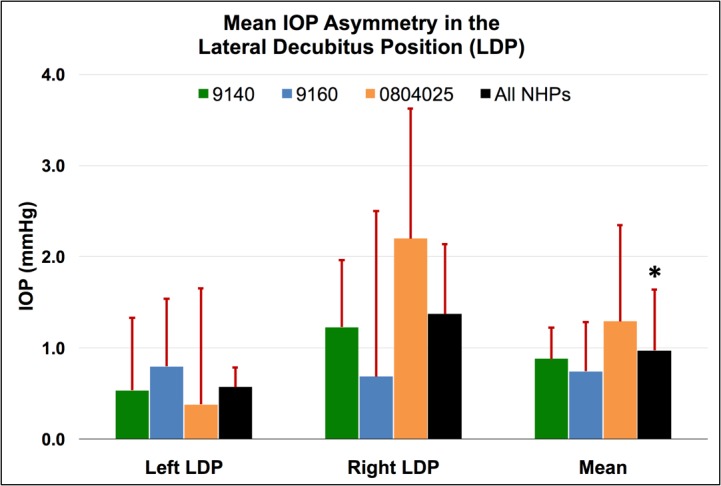
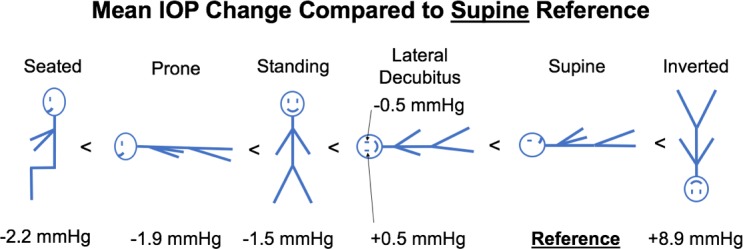
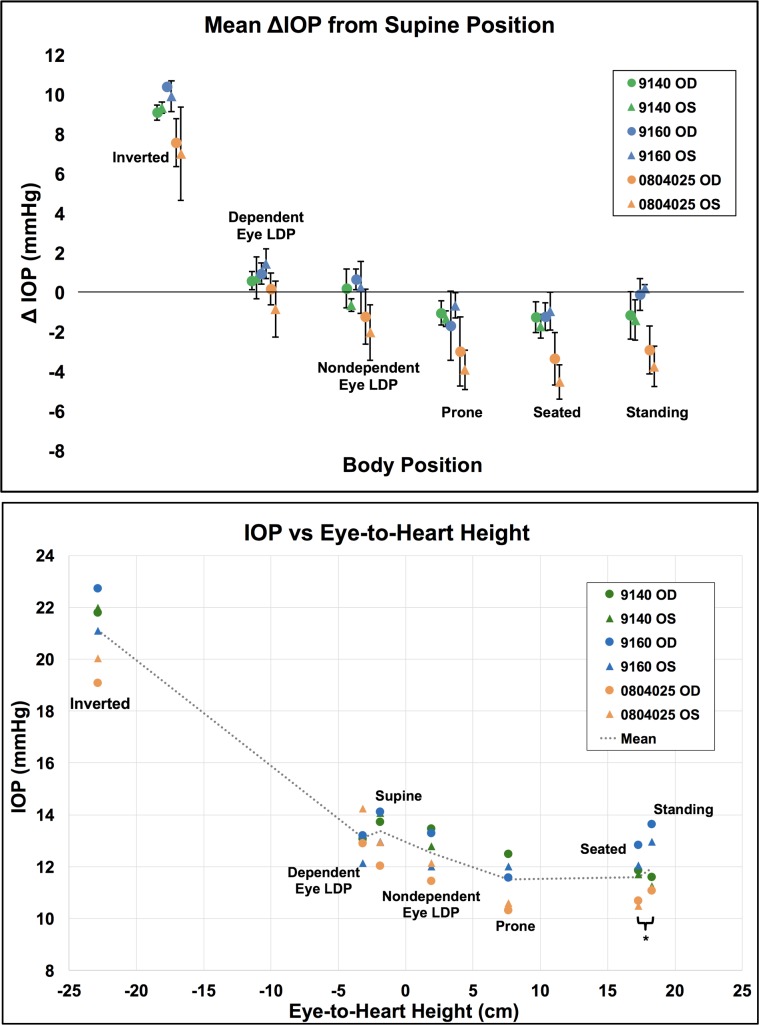
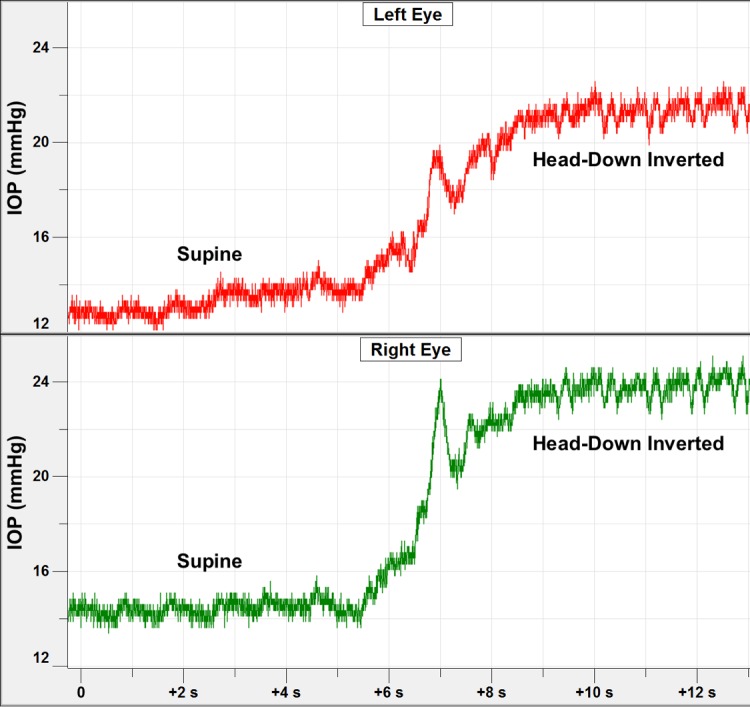
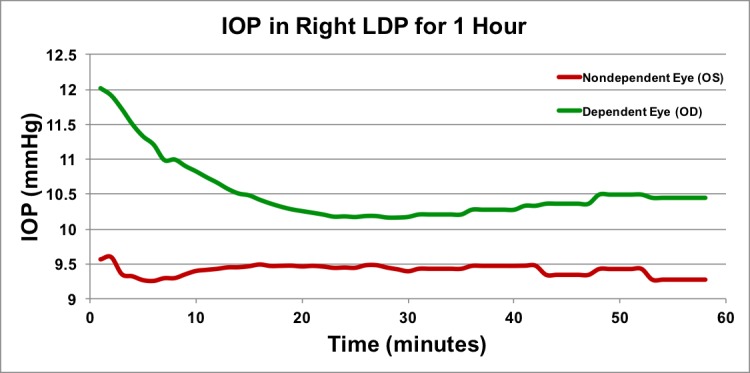
Results: Head-down inversion increased IOP an average of 8.9 mm Hg, compared to the supine reference. In the LDP, IOP decreased an average of 0.5 mm Hg in the nondependent eye (i.e., the higher eye), while the fellow dependent (i.e., lower) eye increased an average of 0.5 mm Hg, compared to supine reference. Standing and seated positions decreased IOP 1.5 and 2.2 mm Hg, respectively, compared with supine reference. IOP changes occurred within 4 to 15 seconds of a body position change, and timing was affected by the speed at which body position was changed. Compared to the IOP in the supine position, the IOP in the inverted, prone, and seated positions was significantly different (P = 0.0313 for all). The IOP in the standing position was not statistically different from the IOP in the supine position (P = 0.094). In addition, the IOP was significantly different between the nondependent eye and the dependent eye in the LDPs compared to the supine position (P = 0.0313).
Conclusions: Body position has a significant effect on IOP and those changes persist over time.
Figures
References
-
- Kim KN, Jeoung JW, Park KH, Kim DM, Ritch R. . Relationship between preferred sleeping position and asymmetric visual field loss in open-angle glaucoma patients. Am J Ophthalmol. 2014; 157: 739– 745. - PubMed
-
- Krieglstein GK, Waller WK, Leydhecker W. . The vascular basis of the positional influence on the intraocular pressure. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1978; 206: 99– 106. - PubMed
-
- Eklund A, Johannesson G, Johansson E,et al. . The pressure difference between eye and brain changes with posture. Ann Neurol. 2016; 80: 269– 276. - PubMed
-
- Cook JA, Botello AP, Elders A,et al. . Systematic review of the agreement of tonometers with Goldmann applanation tonometry. Ophthalmology. 2012; 119: 1552– 1557. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
