

Quantifying the Arousal Threshold Using Polysomnography in Obstructive Sleep Apnea
- PMID: 29228393
- PMCID: PMC5804982
- DOI: 10.1093/sleep/zsx183
Quantifying the Arousal Threshold Using Polysomnography in Obstructive Sleep Apnea
Abstract
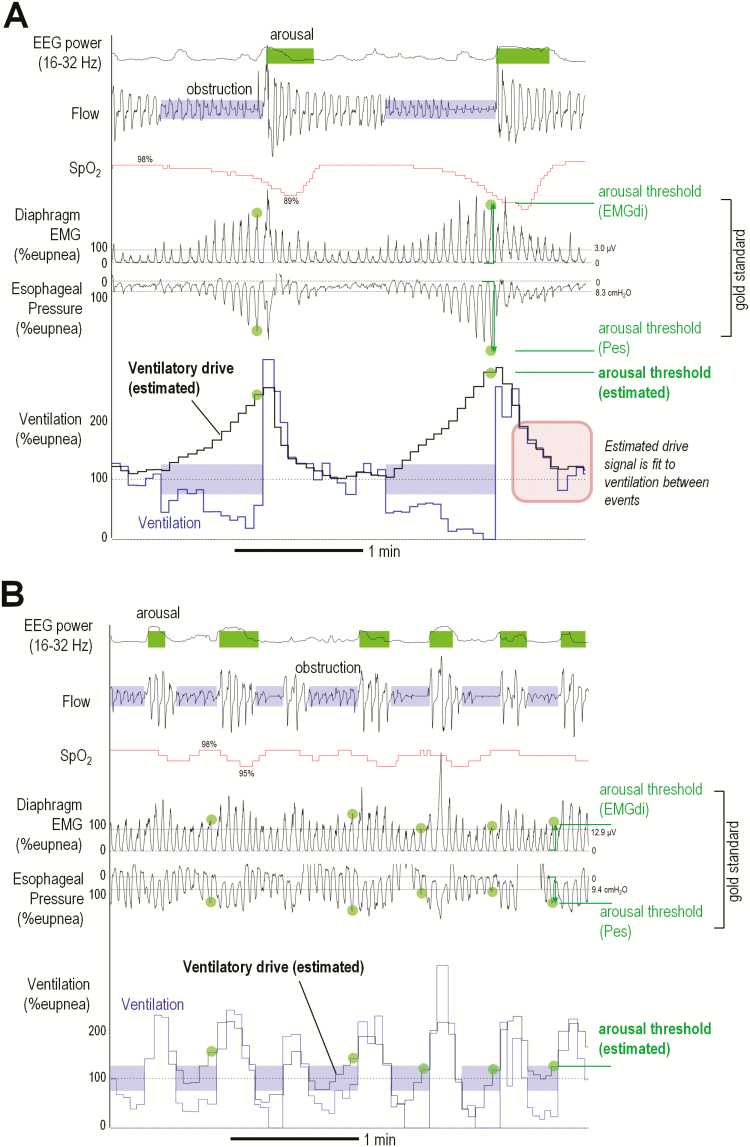
Study objectives: Precision medicine for obstructive sleep apnea (OSA) requires noninvasive estimates of each patient's pathophysiological "traits." Here, we provide the first automated technique to quantify the respiratory arousal threshold-defined as the level of ventilatory drive triggering arousal from sleep-using diagnostic polysomnographic signals in patients with OSA.
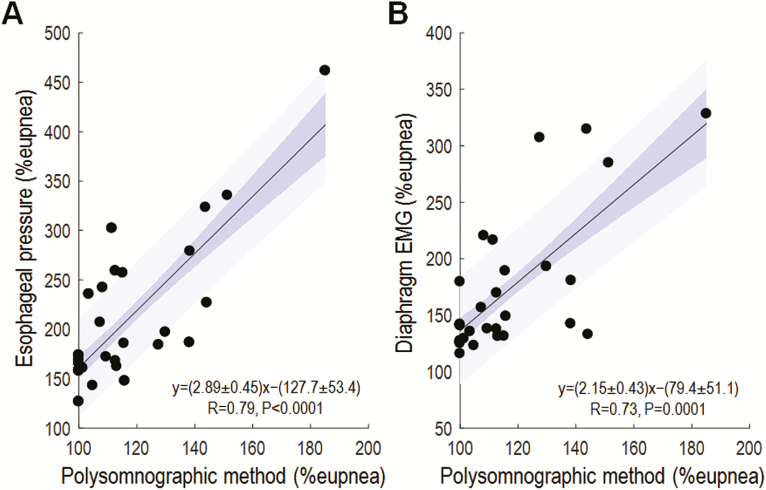
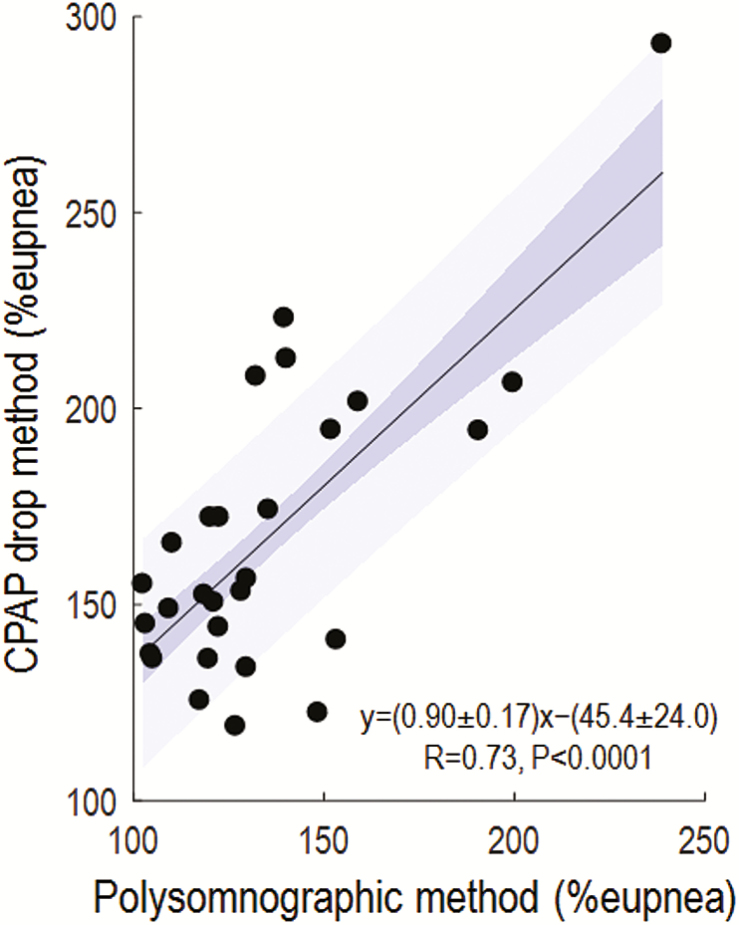
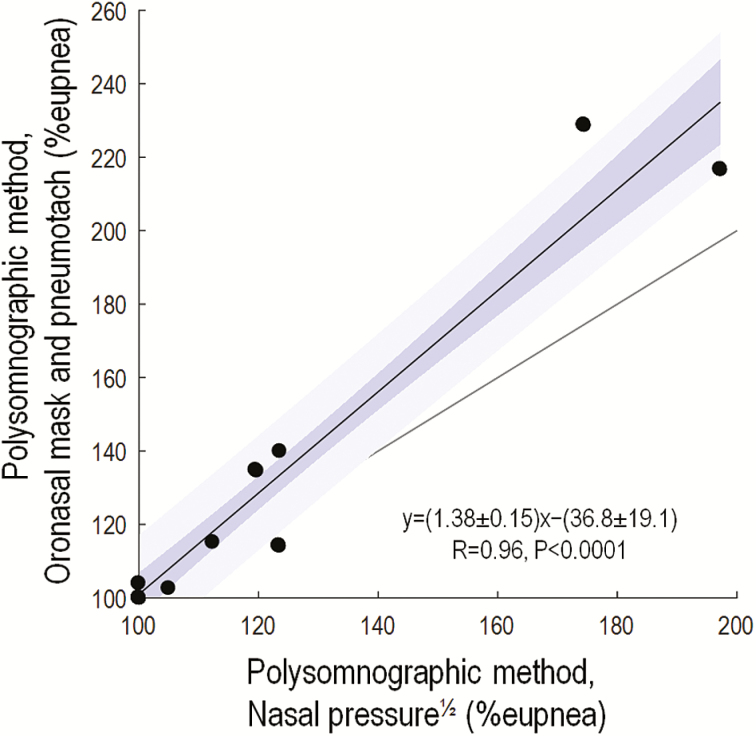
Methods: Ventilatory drive preceding clinically scored arousals was estimated from polysomnographic studies by fitting a respiratory control model (Terrill et al.) to the pattern of ventilation during spontaneous respiratory events. Conceptually, the magnitude of the airflow signal immediately after arousal onset reveals information on the underlying ventilatory drive that triggered the arousal. Polysomnographic arousal threshold measures were compared with gold standard values taken from esophageal pressure and intraoesophageal diaphragm electromyography recorded simultaneously (N = 29). Comparisons were also made to arousal threshold measures using continuous positive airway pressure (CPAP) dial-downs (N = 28). The validity of using (linearized) nasal pressure rather than pneumotachograph ventilation was also assessed (N = 11).
Results: Polysomnographic arousal threshold values were correlated with those measured using esophageal pressure and diaphragm EMG (R = 0.79, p < .0001; R = 0.73, p = .0001), as well as CPAP manipulation (R = 0.73, p < .0001). Arousal threshold estimates were similar using nasal pressure and pneumotachograph ventilation (R = 0.96, p < .0001).
Conclusions: The arousal threshold in patients with OSA can be estimated using polysomnographic signals and may enable more personalized therapeutic interventions for patients with a low arousal threshold.
Keywords: arousability; endotype; pathophysiology; personalized medicine.
© Sleep Research Society 2017. Published by Oxford University Press on behalf of the Sleep Research Society. All rights reserved. For permissions, please e-mail journals.permissions@oup.com.
Figures
References
-
- Gleeson K, Zwillich CW, White DP. The influence of increasing ventilatory effort on arousal from sleep. Am Rev Respir Dis. 1990; 142(2): 295–300. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
