

Treatment with Botulinum toxin A in a total population of children with cerebral palsy - a retrospective cohort registry study
- PMID: 29228927
- PMCID: PMC5725838
- DOI: 10.1186/s12891-017-1880-y
Treatment with Botulinum toxin A in a total population of children with cerebral palsy - a retrospective cohort registry study
Abstract
Background: Botulinum toxin A (BTX-A) has been used to reduce spasticity in children with cerebral palsy (CP) for decades. The purpose of this study was to analyze to what extent BTX-A treatment was used to treat spasticity in a total population of children with CP. We investigated 1) the use of BTX-A in relation to age, sex, and Gross Motor Function Classification System (GMFCS) level, 2) the most common muscle groups treated with BTX-A in relation to the same variables, and 3) changes in the proportions of children treated with BTX-A between two time points (2010 and 2015).
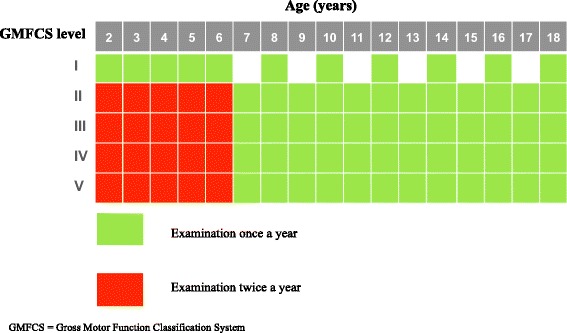
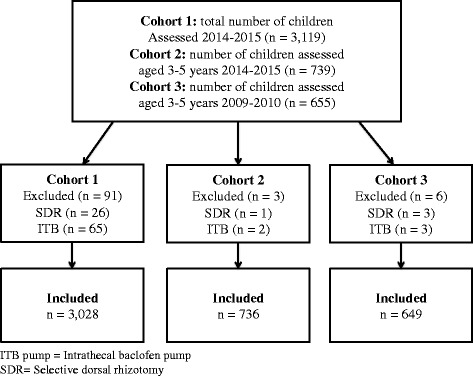
Methods: The study was based on data from CPUP, a combined Swedish follow-up program and national healthcare registry, comprising >95% of all children with CP in Sweden. The participants (N = 3028) were born in 2000 or later. Potential BTX-A treatment and treated muscle groups were included from all CPUP assessments recorded in the registry in 2014-2015. In Aim 3, BTX-A administration in 3-5 year-olds at two time points was assessed. Crosstabs and 95% confidence intervals (CIs) for binominal proportions were calculated and logistic regression was used to regress age, sex, and GMFCS level on BTX-A treatment. Muscle groups treated with BTX-A were assessed using crosstabs and 95% CIs. Proportional change in BTX-A treatment over a 5-year period was analyzed using chi-square.
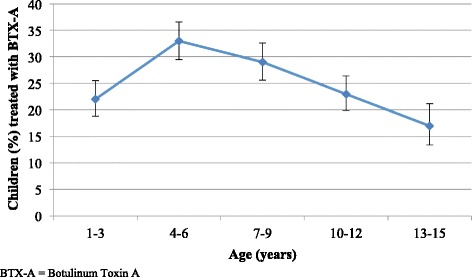
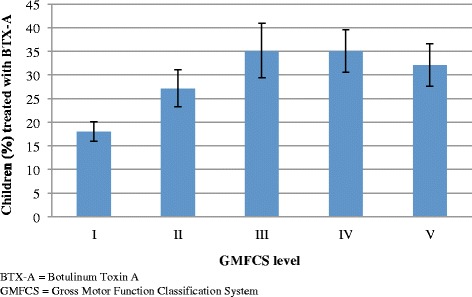
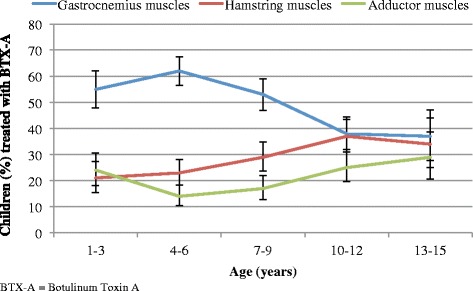
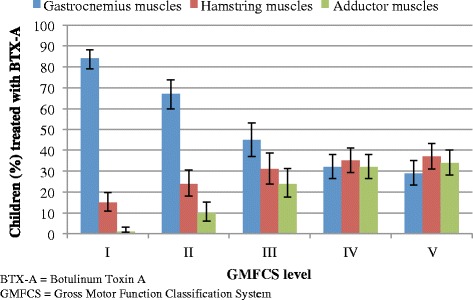
Results: We included 3028 children (57% boys; median age 7 years) of whom 26% received BTX-A. Significantly more boys (28%) than girls (23%) received BTX-A (OR = 1.25, [95% CI 1.05-1.48]). Significant differences were found for age and GMFCS levels; 4-6 year-olds and those at GMFCS III-IV were more likely to receive BTX-A. BTX-A treatment in the gastrocnemius muscle was most common in the 4-6 year-olds and at GMFCS I-III, whereas treatment of the hamstring and adductor muscles was more common in older children and at GMFCS IV-V. No significant change in the proportion of BTX-A administered in 2010 and 2015 was demonstrated.
Conclusions: BTX-A treatment differed based on age, sex, and GMFCS level. Proportion of BTX-A treatment in Sweden has remained stable during the past five years.
Keywords: Age; Botulinum toxin a; CPUP; Cerebral palsy; GMFCS level; Registry; Sex; Spasticity.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Ethics Board at Lund University (LU 443–99, revised 2009), and permission was obtained to extract data from the CPUP registry. Verbal consent to use data for research was provided by all families participating in CPUP.
Consent for publication
Not applicable. This study is based on aggregated data from all children reported to CPUP, Swedish Cerebral Palsy Surveillance Program and National Healthcare Registry.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Miller F. Cerebral Palsy. Springer Publications, New York; 2005. PP 107–108. ISBN 0–387–20437–7.
-
- Hägglund G, Wagner P. Spasticity of the gastrosoleus muscle is related to the development of reduced passive dorsiflexion of the ankle in children with cerebral palsy: a registry analysis of 2,796 examinations in 355 children. Acta Orthop. 2011;82(6):744–748. doi: 10.3109/17453674.2011.618917. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
