

Virtual bronchoscopic navigation without X-ray fluoroscopy to diagnose peripheral pulmonary lesions: a randomized trial
- PMID: 29228929
- PMCID: PMC5725971
- DOI: 10.1186/s12890-017-0531-2
Virtual bronchoscopic navigation without X-ray fluoroscopy to diagnose peripheral pulmonary lesions: a randomized trial
Abstract
Background: Transbronchial biopsy for peripheral pulmonary lesions is generally performed under X-ray fluoroscopy. Virtual bronchoscopic navigation (VBN) is a method in which virtual images of the bronchial route to the lesion are produced based on CT images obtained before VBN, and the bronchoscope is guided using these virtual images, improving the diagnostic yield of peripheral pulmonary lesions. VBN has the possibility of eliminating the need for X-ray fluoroscopy in the bronchoscopic diagnosis of peripheral lesions. To determine whether VBN can be a substitute for X-ray fluoroscopy, a randomized multicenter trial (non-inferiority trial) was performed in VBN and X-ray fluoroscopy (XRF) -assisted groups.
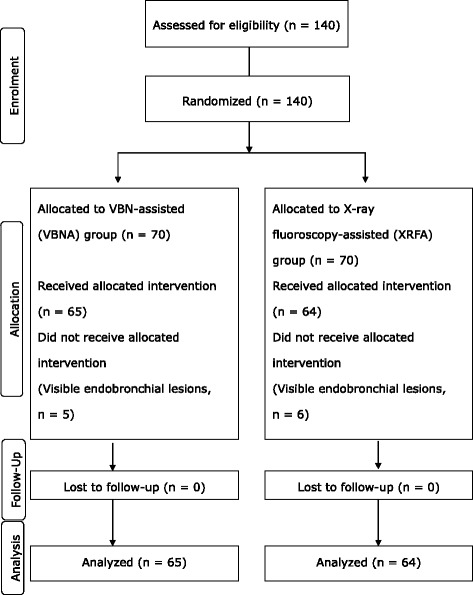
Methods: The non-inferiority margin in the VBN-assisted group compared with the XRF-assisted group was set at 15%. The subjects consisted of 140 patients with peripheral pulmonary lesions with a mean diameter > 3 cm. In the VBN-assisted group, the bronchoscope was guided to the lesion using a VBN system without X-ray fluoroscopy. In the XRF-assisted group, the same bronchoscope was guided to the lesion under X-ray fluoroscopy. Subsequently, in both groups, the lesion was visualized using endobronchial ultrasonography with a guide sheath (EBUS/GS), and biopsy was performed. In this serial procedure, X-ray fluoroscopy was not used in the VBNA group.
Results: The subjects of analysis consisted of 129 patients. The diagnostic yield was 76.9% (50/65) in the VBN-assisted group and 85.9% (55/64) in the XRF-assisted group. The difference in the diagnostic yield between the two groups was -9.0% (95% confidence interval: -22.3% ~ 4.3%). The non-inferiority of the VBN-assisted group could not be confirmed. The rate of visualizing lesions by EBUS was 95.4% (62/65) in the VBN-assisted group and 96.9% (62/64) in the XRF-assisted group, being high in both groups.
Conclusions: On EBUS/GS, a bronchoscope and biopsy instruments may be guided to the lesions using VBN without X-ray fluoroscopy, but X-ray fluoroscopy is necessary to improve the accuracy of sample collection from lesions. During transbronchial biopsy for peripheral pulmonary lesions, VBN cannot be a substitute for X-ray fluoroscopy.
Trial registration: UMIN-CTR (UMIN000001710); registered 16 February 2009.
Keywords: Bronchoscopy; Endobronchial ultrasonography; Guide sheath; Lung cancer; Peripheral pulmonary lesion; Transbronchial biopsy; Virtual bronchoscopic navigation; X-ray fluoroscopy.
Conflict of interest statement
Ethics approval and consent to participate
The review boards of each participating institution approved all study protocols (Ethics Review Committee of Gifu Prefectural General Medical Center, 2008-14; Research ethics committee of Fukushima medical university, 837; Research ethics committee of Hokkaido University School of Medicine, 008-0115; Ethics Review Committee of National Hospital Organization Hokkaido Cancer Center, 20-7; Institutional Review Board of University of Fukui Hospital, 2009-819) and all patients provided written informed consent to participate according to the Declaration of Helsinki.
Consent for publication
Not Applicable.
Competing interests
Dr. Fumihiro Asano has received speaker fees from Olympus Medical Systems as invited guests to academic medical meetings. All other authors declare that they have no conflict of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Bronchoscopy Using Virtual Navigation and Endobronchial Ultrasonography with a Guide Sheath (EBUS-GS) with or without Fluoroscopy for Peripheral Pulmonary Lesions.Kobe J Med Sci. 2018 Mar 27;63(4):E99-E104. Kobe J Med Sci. 2018. PMID: 29955020 Free PMC article. Clinical Trial.
-
Virtual bronchoscopic navigation combined with endobronchial ultrasound to diagnose small peripheral pulmonary lesions: a randomised trial.Thorax. 2011 Dec;66(12):1072-7. doi: 10.1136/thx.2010.145490. Epub 2011 Jul 11. Thorax. 2011. PMID: 21749984 Free PMC article. Clinical Trial.
-
[A study of the diagnostic value of endobronchial ultrasound guide sheath transbronchial lung biopsy combined with virtual bronchoscopic navigation in peripheral pulmonary lesions].Zhonghua Jie He He Hu Xi Za Zhi. 2016 Jul;39(7):509-13. doi: 10.3760/cma.j.issn.1001-0939.2016.07.004. Zhonghua Jie He He Hu Xi Za Zhi. 2016. PMID: 27430920 Clinical Trial. Chinese.
-
Virtual bronchoscopic navigation for peripheral pulmonary lesions.Respiration. 2014;88(5):430-40. doi: 10.1159/000367900. Epub 2014 Oct 1. Respiration. 2014. PMID: 25402610 Review.
-
Competence in navigation and guided transbronchial biopsy for peripheral pulmonary lesions.Panminerva Med. 2019 Sep;61(3):280-289. doi: 10.23736/S0031-0808.18.03568-1. Epub 2018 Oct 31. Panminerva Med. 2019. PMID: 30394715 Review.
Cited by
-
Radial-EBUS and virtual bronchoscopy planner for peripheral lung cancer diagnosis: How it became the first-line endoscopic procedure.Thorac Cancer. 2022 Oct;13(20):2854-2860. doi: 10.1111/1759-7714.14629. Epub 2022 Aug 29. Thorac Cancer. 2022. PMID: 36054681 Free PMC article.
-
Study design for a multicenter, randomized controlled trial evaluating the diagnostic value of ultrathin bronchoscope compared to thin bronchoscope without fluoroscopy for peripheral pulmonary lesions.J Thorac Dis. 2022 May;14(5):1663-1673. doi: 10.21037/jtd-22-20. J Thorac Dis. 2022. PMID: 35693609 Free PMC article.
-
Ultrathin bronchoscope combined with virtual bronchoscopic navigation and endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions with or without fluoroscopy: A randomized trial.Thorac Cancer. 2021 Jun;12(12):1864-1872. doi: 10.1111/1759-7714.13995. Epub 2021 May 6. Thorac Cancer. 2021. PMID: 33956409 Free PMC article. Clinical Trial.
-
Development of the Korean Association for Lung Cancer Clinical Practice Guidelines: Recommendations on Radial Probe Endobronchial Ultrasound for Diagnosing Lung Cancer - An Updated Meta-Analysis.Cancer Res Treat. 2024 Apr;56(2):464-483. doi: 10.4143/crt.2023.749. Epub 2023 Nov 29. Cancer Res Treat. 2024. PMID: 38037321 Free PMC article.
-
Virtual bronchoscopic navigation versus non-virtual bronchoscopic navigation assisted bronchoscopy for the diagnosis of peripheral pulmonary lesions: a systematic review and meta-analysis.Ther Adv Respir Dis. 2021 Jan-Dec;15:17534666211017048. doi: 10.1177/17534666211017048. Ther Adv Respir Dis. 2021. PMID: 34057861 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
