

Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes
- PMID: 29228951
- PMCID: PMC5725835
- DOI: 10.1186/s13054-017-1891-y
Hypovitaminosis C and vitamin C deficiency in critically ill patients despite recommended enteral and parenteral intakes
Abstract
Background: Vitamin C is an essential water-soluble nutrient which cannot be synthesised or stored by humans. It is a potent antioxidant with anti-inflammatory and immune-supportive roles. Previous research has indicated that vitamin C levels are depleted in critically ill patients. In this study we have assessed plasma vitamin C concentrations in critically ill patients relative to infection status (septic shock or non-septic) and level of inflammation (C-reactive protein concentrations). Vitamin C status was also assessed relative to daily enteral and parenteral intakes to determine if standard intensive care unit (ICU) nutritional support is adequate to meet the vitamin C needs of critically ill patients.
Methods: Forty-four critically ill patients (24 with septic shock, 17 non-septic, 3 uncategorised) were recruited from the Christchurch Hospital Intensive Care Unit. We measured concentrations of plasma vitamin C and a pro-inflammatory biomarker (C-reactive protein) daily over 4 days and calculated patients' daily vitamin C intake from the enteral or total parenteral nutrition they received. We compared plasma vitamin C and C-reactive protein concentrations between septic shock and non-septic patients over 4 days using a mixed effects statistical model, and we compared the vitamin C status of the critically ill patients with known vitamin C bioavailability data using a four-parameter log-logistic response model.
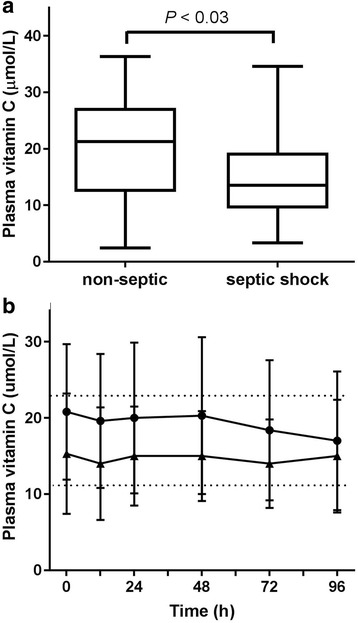
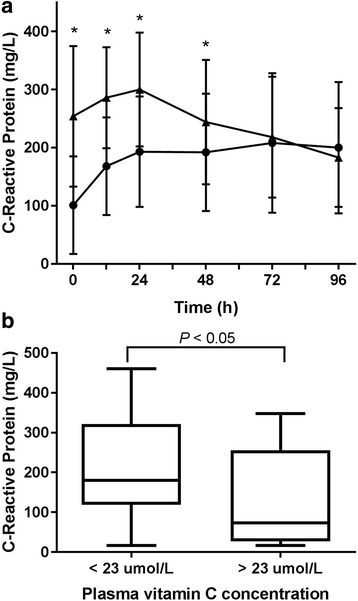
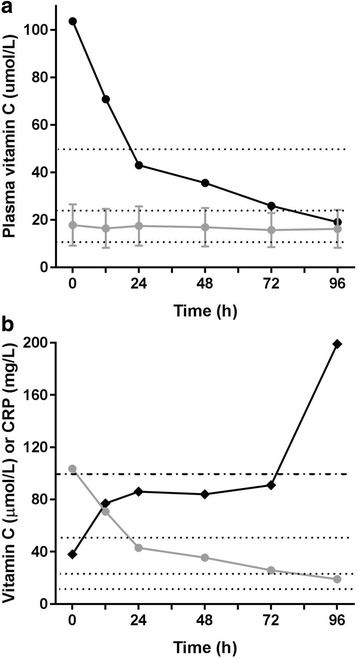
Results: Overall, the critically ill patients exhibited hypovitaminosis C (i.e., < 23 μmol/L), with a mean plasma vitamin C concentration of 17.8 ± 8.7 μmol/L; of these, one-third had vitamin C deficiency (i.e., < 11 μmol/L). Patients with hypovitaminosis C had elevated inflammation (C-reactive protein levels; P < 0.05). The patients with septic shock had lower vitamin C concentrations and higher C-reactive protein concentrations than the non-septic patients (P < 0.05). Nearly 40% of the septic shock patients were deficient in vitamin C, compared with 25% of the non-septic patients. These low vitamin C levels were apparent despite receiving recommended intakes via enteral and/or parenteral nutritional therapy (mean 125 mg/d).
Conclusions: Critically ill patients have low vitamin C concentrations despite receiving standard ICU nutrition. Septic shock patients have significantly depleted vitamin C levels compared with non-septic patients, likely resulting from increased metabolism due to the enhanced inflammatory response observed in septic shock.
Keywords: C-reactive protein; Critical illness; Enteral nutrition; Hypovitaminosis C; Intensive care; Parenteral nutrition; Sepsis; Septic shock; Vitamin C.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
All procedures involving human participants were approved by the Southern Health and Disability Ethics Committee (15/STH/36). Proxy consent was obtained from the treating physician in consultation with family members when patient consent was not possible. Consent from patients was sought as soon as they had sufficiently recovered.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Comment in
-
The adrenal-vitamin C axis: from fish to guinea pigs and primates.Crit Care. 2019 Jan 28;23(1):29. doi: 10.1186/s13054-019-2332-x. Crit Care. 2019. PMID: 30691525 Free PMC article. No abstract available.
-
A new clinical trial to test high-dose vitamin C in patients with COVID-19.Crit Care. 2020 Apr 7;24(1):133. doi: 10.1186/s13054-020-02851-4. Crit Care. 2020. PMID: 32264963 Free PMC article. No abstract available.
References
-
- Nishikimi M, Fukuyama R, Minoshima S, Shimizu N, Yagi K. Cloning and chromosomal mapping of the human nonfunctional gene for l-gulono-γ-lactone oxidase, the enzyme for l-ascorbic acid biosynthesis missing in man. J Biol Chem. 1994;269(18):13685–8. - PubMed
-
- Carr A, Frei B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999;13(9):1007–24. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
