

Impact of prematurity and nutrition on the developing gut microbiome and preterm infant growth
- PMID: 29228972
- PMCID: PMC5725645
- DOI: 10.1186/s40168-017-0377-0
Impact of prematurity and nutrition on the developing gut microbiome and preterm infant growth
Abstract
Background: Identification of factors that influence the neonatal gut microbiome is urgently needed to guide clinical practices that support growth of healthy preterm infants. Here, we examined the influence of nutrition and common practices on the gut microbiota and growth in a cohort of preterm infants.
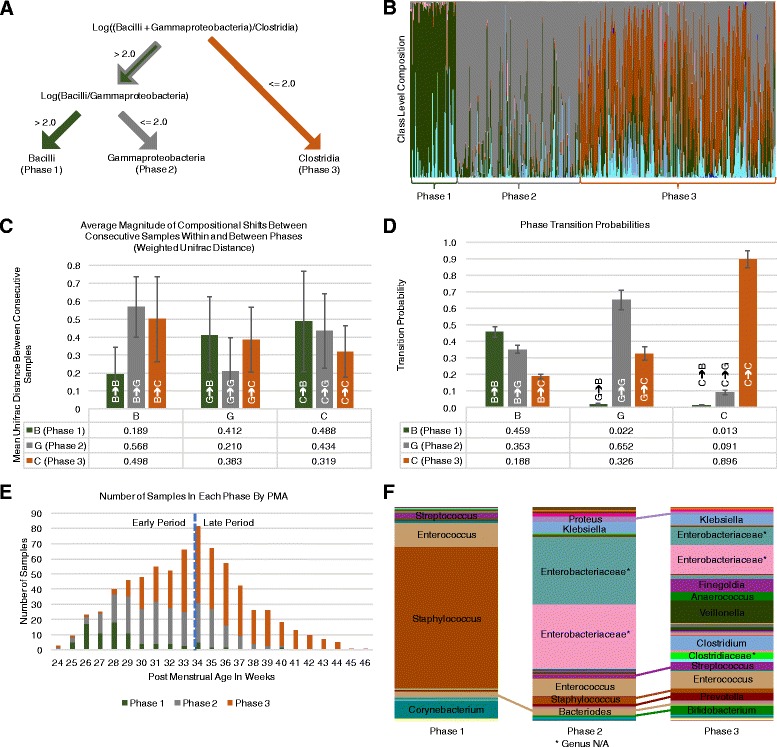
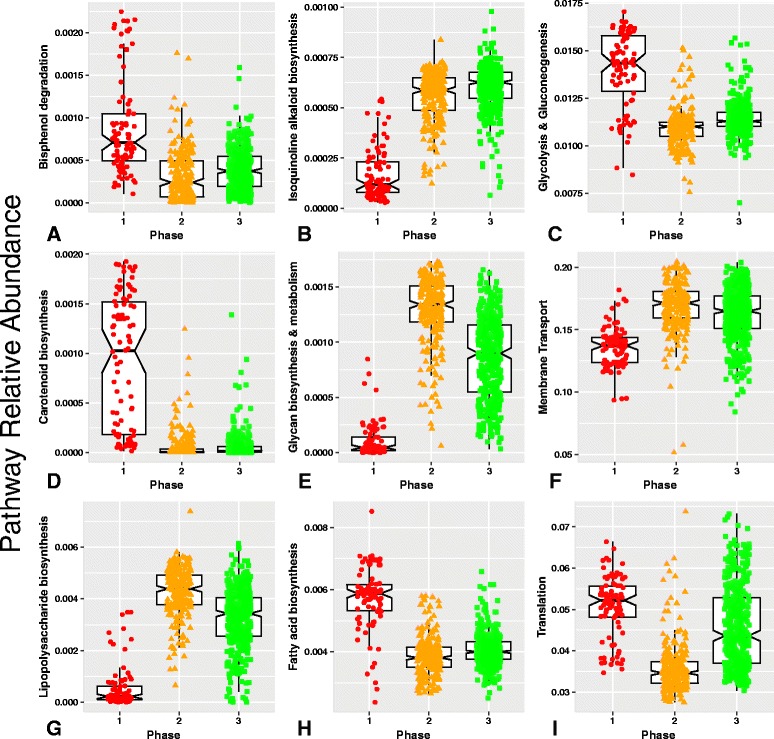
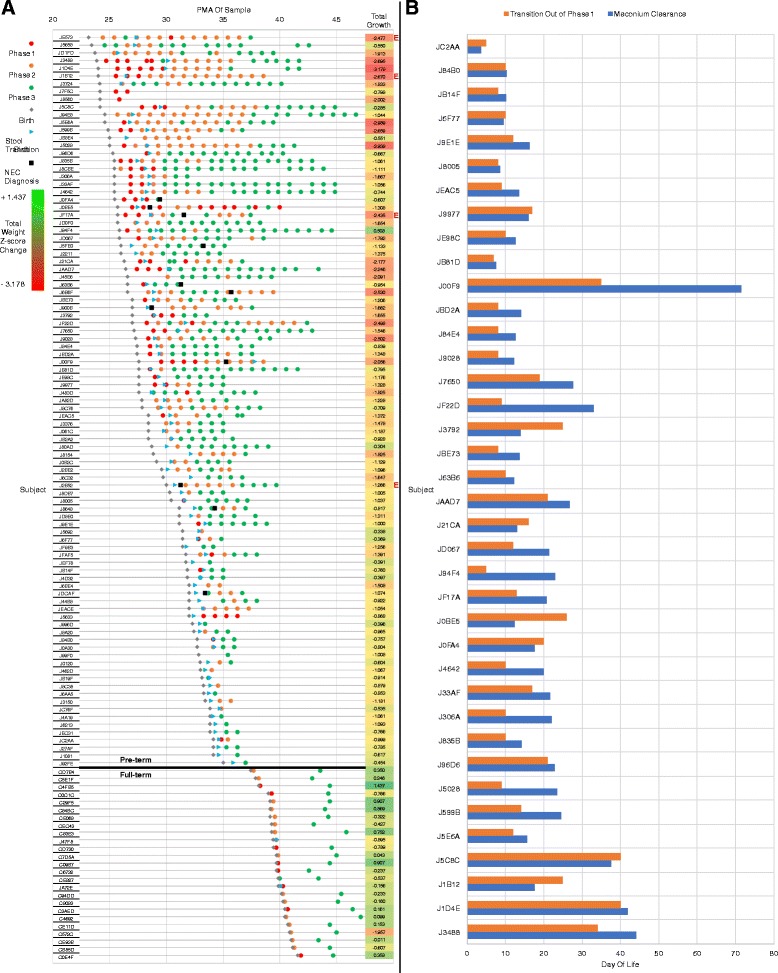
Results: With weekly gut microbiota samples spanning postmenstrual age (PMA) 24 to 46 weeks, we developed two models to test associations between the microbiota, nutrition and growth: a categorical model with three successive microbiota phases (P1, P2, and P3) and a model with two periods (early and late PMA) defined by microbiota composition and PMA, respectively. The more significant associations with phase led us to use a phase-based framework for the majority of our analyses. Phase transitions were characterized by rapid shifts in the microbiota, with transition out of P1 occurring nearly simultaneously with the change from meconium to normal stool. The rate of phase progression was positively associated with gestational age at birth, and delayed transition to a P3 microbiota was associated with growth failure. We found distinct bacterial metabolic functions in P1-3 and significant associations between nutrition, microbiota phase, and infant growth.
Conclusion: The phase-dependent impact of nutrition on infant growth along with phase-specific metabolic functions suggests a pioneering potential for improving growth outcomes by tailoring nutrient intake to microbiota phase.
Keywords: Gut microbiota; Infant growth; Meconium; Nutrition; Phase transition; Preterm infants.
Conflict of interest statement
Ethics approval and consent to participate
Written informed consent was obtained from a parent or guardian of all participating infants. The institutional review board at the University of Rochester School of Medicine and Strong Memorial Hospital approved the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Blanton LV, Charbonneau MR, Salih T, Barratt MJ, Venkatesh S, Ilkaveya O, Subramanian S, Manary MJ, Trehan I, Jorgensen JM, et al. MICROBIOME gut bacteria that prevent growth impairments transmitted by microbiota from malnourished children. Science. 2016;351(6275):830–U857. doi: 10.1126/science.aad3311. - DOI - PMC - PubMed
-
- Kostic AD, Gevers D, Siljander H, Vatanen T, Hyotylainen T, Hamalainen AM, Peet A, Tillmann V, Poho P, Mattila I, et al. The dynamics of the human infant gut microbiome in development and in progression toward type 1 diabetes. Cell Host Microbe. 2015;17(2):260–273. doi: 10.1016/j.chom.2015.01.001. - DOI - PMC - PubMed
-
- La Rosa PS, Warner BB, Zhou Y, Weinstock GM, Sodergren E, Hall-Moore CM, Stevens HJ, Bennett WE, Jr, Shaikh N, Linneman LA, et al. Patterned progression of bacterial populations in the premature infant gut. Proc Natl Acad Sci U S A. 2014;111(34):12522–12527. doi: 10.1073/pnas.1409497111. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
