

Immediate/Early vs. Delayed Invasive Strategy for Patients with Non-ST-Segment Elevation Acute Coronary Syndromes: A Systematic Review and Meta-Analysis
- PMID: 29230180
- PMCID: PMC5712112
- DOI: 10.3389/fphys.2017.00952
Immediate/Early vs. Delayed Invasive Strategy for Patients with Non-ST-Segment Elevation Acute Coronary Syndromes: A Systematic Review and Meta-Analysis
Abstract
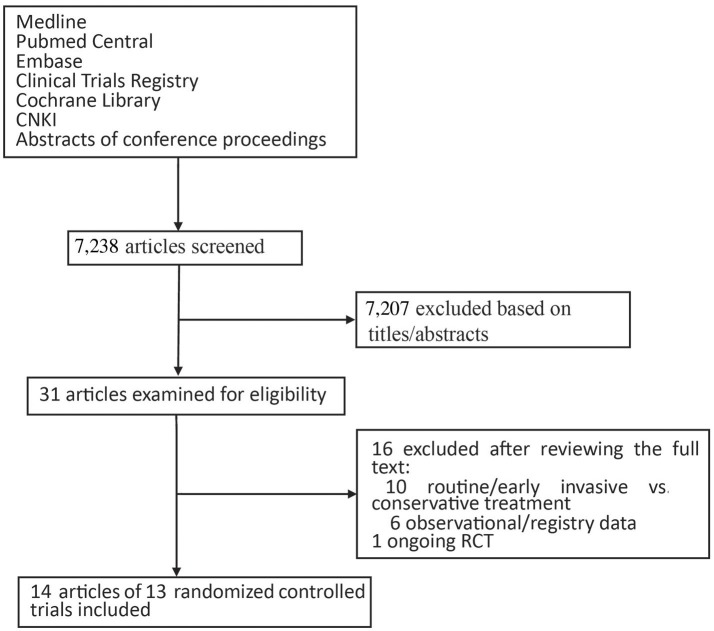
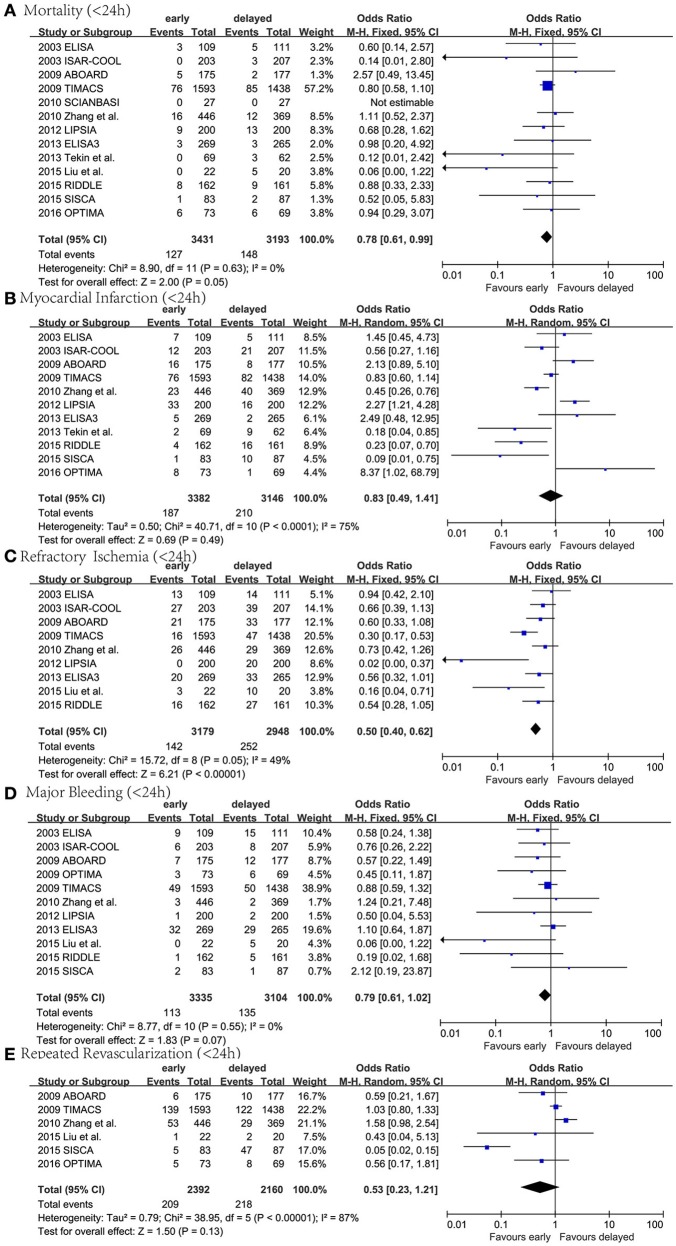
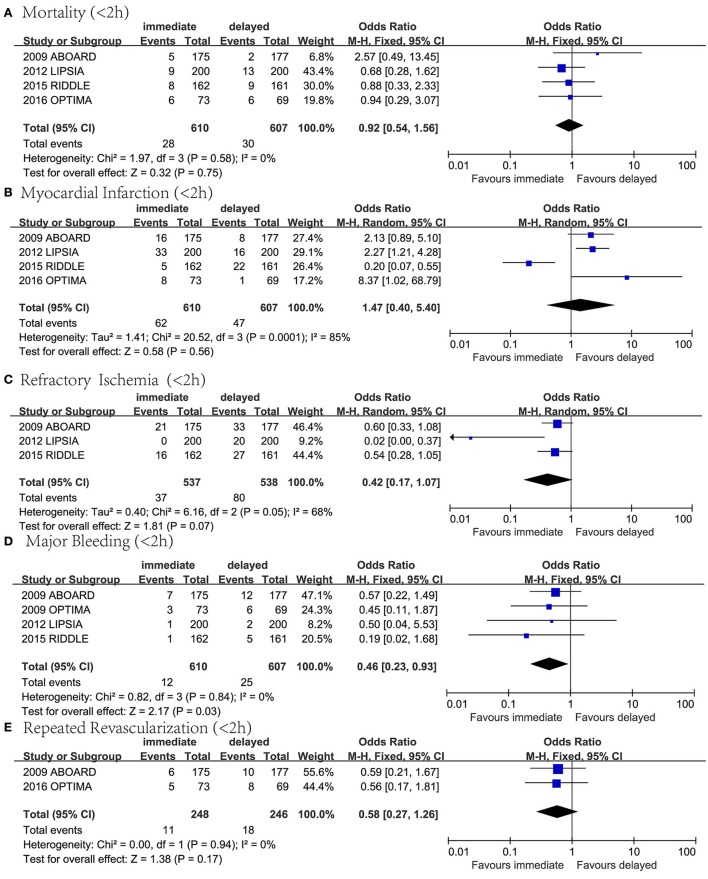
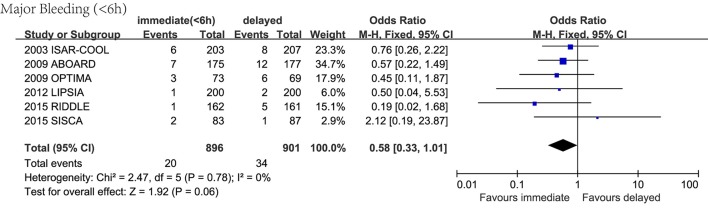
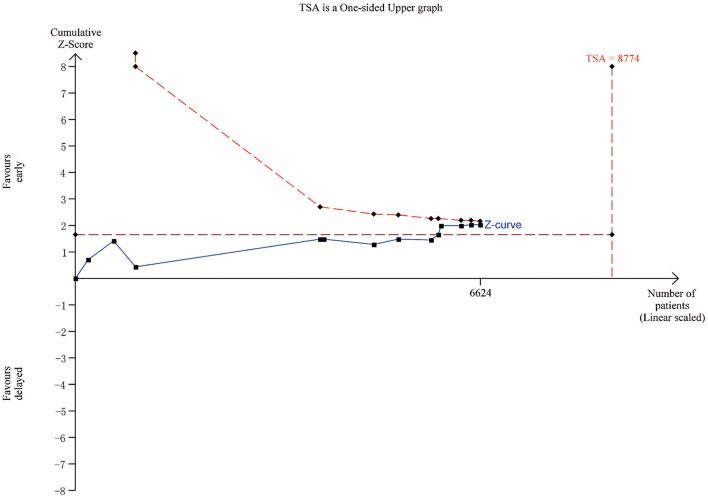
Invasive coronary revascularization has been shown to improve prognoses in patients with non-ST-segment elevation acute coronary syndromes (NSTE-ACS), but the optimal timing of intervention remains unclear. This meta-analysis is to evaluate the outcomes in immediate (<2 h), early (<24 h), and delayed invasive group and find out which is the optimal timing of intervention in NSTE-ACS patients. Studies were identified through electronic literature search of Medline, PubMed Central, Embase, the Cochrane Library, and CNKI. Data were extracted for populations, interventions, outcomes, and risk of bias. All-cause mortality was the pre-specified primary end point. The longest follow-up available in each study was chosen. The odds ratio (OR) with 95% CI was the effect measure. The fixed or random effect pooled measure was selected based on the heterogeneity test among studies. In the comparison between early and delayed intervention, we found that early intervention led to a statistical significant decrease in mortality rate (n = 6,624; OR 0.78, 95% CI: 0.61-0.99) and refractory ischemia (n = 6,127; OR 0.50, 95% CI: 0.40-0.62) and a non-significant decrease in myocardial infarction (MI), major bleeding and revascularization. In the analysis comparing immediate and delayed invasive approach, we found that immediate intervention significantly reduced major bleeding (n = 1,217; OR 0.46, 95% CI: 0.23-0.93) but led to a non-significant decrease in mortality rate, refractory ischemia and revascularization and a non-significant increase in MI. In conclusion, early invasive strategy may lead to a lower mortality rate and reduce the risk of refractory ischemia, while immediate invasive therapy shows a benefit in reducing the risk of major bleeding.
Keywords: intervention; invasive strategy; major bleeding; meta-analysis; mortality rate; non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
Figures
References
-
- Abbas A. E., Brodie B., Dixon S., Marsalese D., Brewington S., O'Neill W. W., et al. (2005). Incidence and prognostic impact of gastrointestinal bleeding after percutaneous coronary intervention for acute myocardial infarction. Am. J. Cardiol. 96, 173–176. 10.1016/j.amjcard.2005.03.038 - DOI - PubMed
-
- Anderson J. L., Adams C. D., Antman E. M., Bridges C. R., Califf R. M., Casey D. E., Jr., et al. (2013). 2012 ACCF/AHA focused update incorporated Into the ACCF/AHA 2007 guidelines for the management of patients with unstable Angina/Non-ST-elevation myocardial Infarction: a report of the american college of cardiology foundation/american heart association task force on practice guidelines. J Am. Coll. Cardiol. 61, 179–347. 10.1016/j.jacc.2013.01.014 - DOI - PubMed
-
- Fox K. A., Clayton T. C., Damman P., Pocock S. J., de Winter R. J., Tijssen J. G., et al. (2010). Long-term outcome of a routine vs. selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome. J. Am. Coll Cardiol. 55, 2435–2445. 10.1016/j.jacc.2010.03.007 - DOI - PubMed
-
- Hamm C. W., Bassand J. P., Agewall S., Bax J., Boersma E., Bueno H., et al. (2011). ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 32, 2999–3054. 10.1093/eurheartj/ehr236 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources