

Risks of bleeding and thrombosis in intensive care unit patients with haematological malignancies
- PMID: 29230562
- PMCID: PMC5725397
- DOI: 10.1186/s13613-017-0341-y
Risks of bleeding and thrombosis in intensive care unit patients with haematological malignancies
Abstract
Background: Patients with malignant haematological disease and especially those who require intensive care have an increased risk of bleeding and thrombosis, but none of these data were obtained in ICU patients only. We assessed the incidence of bleeding and thrombotic complications, use of blood products and risk factors for bleeding in an adult population of ICU patients with haematological malignancies.
Methods: We screened all patients with acute leukaemia and myelodysplastic syndrome admitted to a university hospital ICU during 2008-2012. Bleeding in ICU was scored according to the WHO grading system, and risk factors were evaluated using unadjusted and adjusted analyses.
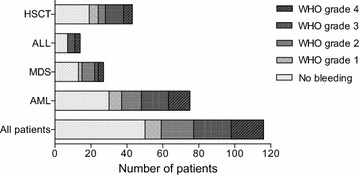
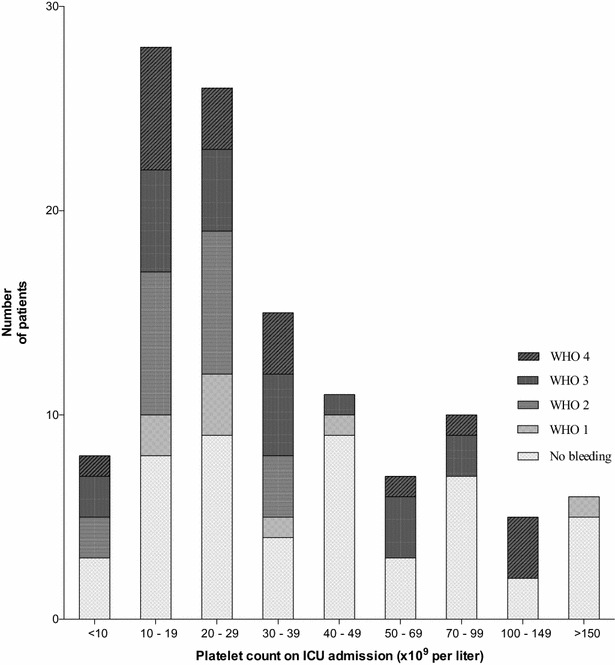
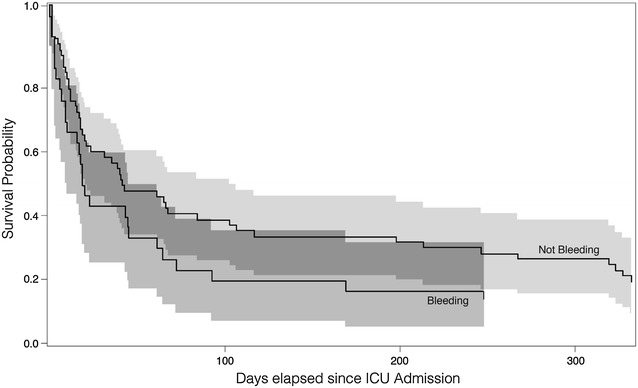
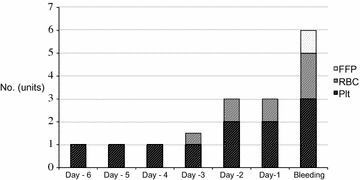
Results: In total, 116 of 129 ICU patients were included; their median length of stay was 7 (IQR 2-16) days. Of these, 66 patients (57%) had at least one bleeding episode in ICU; they bled for 3 (2-6) days and most often from lower and upper airways and upper GI tract. Thirty-nine (59%) of the 66 patients had severe or debilitating (WHO grade 3 or 4) bleeding. The median platelet count on the day of grade 3 or 4 bleeding was 23 × 109 per litre (IQR 13-39). Nine patients (8%) died in ICU following a bleeding episode; five of these had intra-cerebral haemorrhage. Platelet count on admission was associated with subsequent bleeding (adjusted odds ratio 1.18 (95% CI 1.03-1.35) for every 10 × 109 per litre drop in platelet count, p = 0.016). Eleven of the 116 patients (9%) developed a clinically significant thrombosis in ICU, which was the cause of death in four patients. The median platelet count was 20 × 109 per litre (15-48) at the time of thrombosis. The patients received a median of 6 units of red blood cells, 1 unit of fresh frozen plasma and 8 units of platelet concentrates in ICU.
Conclusions: Severe and debilitating bleeding complications were frequent in our ICU patients with haematological malignancies, but thrombosis also occurred in spite of low platelet counts. Platelet count on ICU admission was associated with subsequent bleeding.
Keywords: Bleeding; Haematology; ICU; Intensive care; Leukaemia; Myelodysplastic syndrome; Sepsis; Thrombosis; Transfusion.
Figures
References
-
- Schellongowski P, Staudinger T, Kundi M, et al. Prognostic factors for intensive care unit admission, intensive care outcome, and post-intensive care survival in patients with de novo acute myeloid leukemia: a single center experience. Haematologica. 2011;96(2):231–237. doi: 10.3324/haematol.2010.031583. - DOI - PMC - PubMed
-
- Azoulay E, Mokart D, Pène F, et al. Outcomes of critically ill patients with hematologic malignancies: prospective multicenter data from France and Belgium—a groupe de recherche respiratoire en réanimation onco-hématologique study. J Clin Oncol. 2013;31(22):2810–2818. doi: 10.1200/JCO.2012.47.2365. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
