

The Liver Frailty Index Improves Mortality Prediction of the Subjective Clinician Assessment in Patients With Cirrhosis
- PMID: 29231189
- PMCID: PMC5866923
- DOI: 10.1038/ajg.2017.443
The Liver Frailty Index Improves Mortality Prediction of the Subjective Clinician Assessment in Patients With Cirrhosis
Abstract
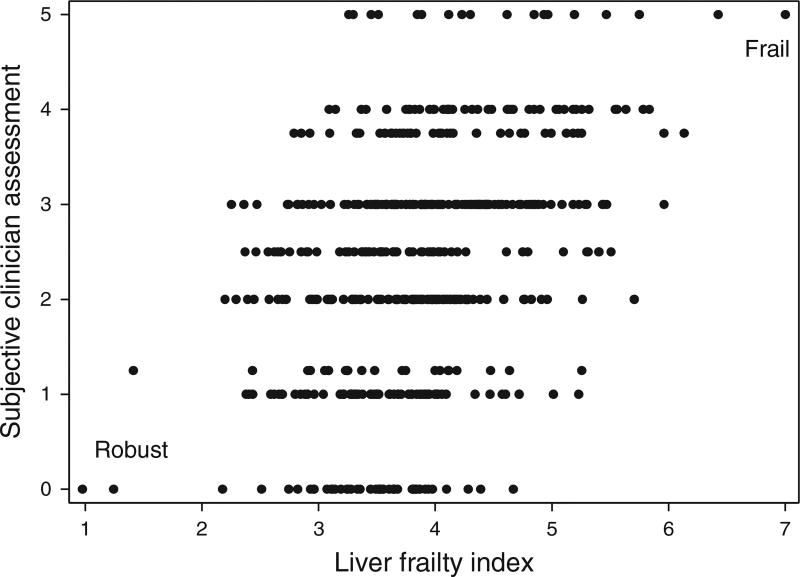
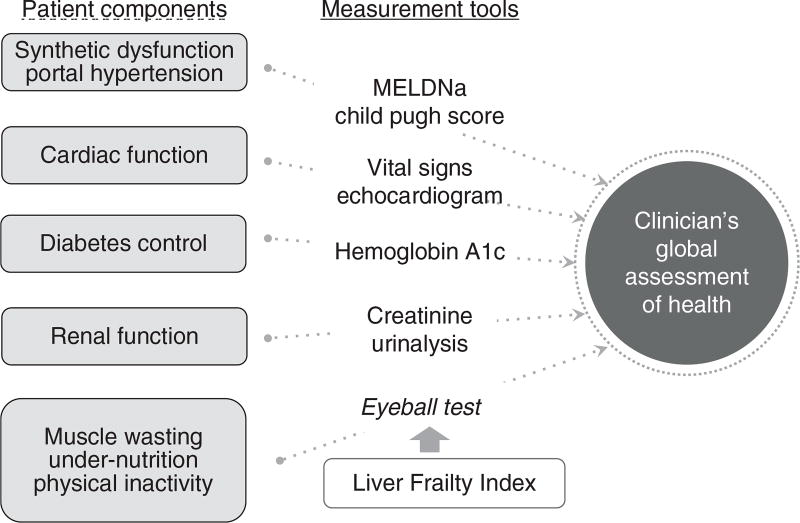
Objectives: Frailty, a critical determinant of health outcomes, is most commonly assessed in patients with cirrhosis by general clinician assessment that is limited by its subjectivity. We aimed to compare the objective Liver Frailty Index (LFI), consisting of three performance-based tests (grip, chair stands, balance), with a subjective hepatologist assessment.
Methods: Outpatients with cirrhosis awaiting liver transplantation (LT) underwent: (1) objective measurement using the LFI and (2) subjective clinician assessment. Spearman's correlation assessed associations between the LFI and clinician assessment; Cox regression with waitlist mortality (death/delisting for sickness); discriminative ability with Concordance(C) statistics. The net reclassification index evaluated the percentage of patients correctly reclassified by adding the LFI to the clinician assessment.
Results: Of the 529 patients with cirrhosis, median LFI was 3.8 (range 1.0-7.0) and clinician assessment was 3 (range 0-5). Correlation between LFI and the clinician assessment was modest (ρ=0.38) with high variability by hepatologist (ρ=0.26-0.70). At a median of 11 months, 102 (19%) died/were delisted. Both the LFI (hazard ratio (HR) 2.2, 95% confidence interval (CI) 1.7-2.9) and clinician assessment (HR 1.6, 95% CI 1.3-1.9) were associated with adjusted waitlist mortality risk (P<0.01). The addition of the LFI to the clinician assessment significantly improved mortality prediction over the clinician assessment alone (0.74 vs. 0.68; P=0.02). Compared with the clinician assessment alone, the addition of the LFI correctly reclassified 34% (95% CI 8-53%) of patients to their correct survival status.
Conclusion: The subjective clinician assessment can predict waitlist mortality in patients with cirrhosis but is subjective and variable by hepatologist. The addition of the LFI to the subjective clinician assessment significantly improved mortality risk prediction, reclassifying 34% of patients. Our data strongly support the incorporation of the objective LFI to anchor our assessments of patients with cirrhosis to enhance our decision-making.
Conflict of interest statement
Figures
References
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:146–56. - PubMed
-
- Weissenborn K, Ruckert N, Hecker H, et al. The number connection tests A and B: interindividual variability and use for the assessment of early hepatic encephalopathy. J Hepatol. 1998;28:646–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
