

Cardiovascular magnetic resonance imaging and clinical performance of somatostatin receptor positron emission tomography in cardiac sarcoidosis
- PMID: 29231290
- PMCID: PMC5880659
- DOI: 10.1002/ehf2.12243
Cardiovascular magnetic resonance imaging and clinical performance of somatostatin receptor positron emission tomography in cardiac sarcoidosis
Abstract
Aims: Cardiac affection constitutes a major limiting condition in systemic sarcoidosis. The primary objective of this study was to investigate the persistence rate of cardiac sarcoid involvement by cardiovascular magnetic resonance (CMR) imaging in patients diagnosed with cardiac sarcoidosis (CS). Moreover, we examined the additional insights into myocardial damage's characteristics gained by somatostatin receptor scintigraphy.
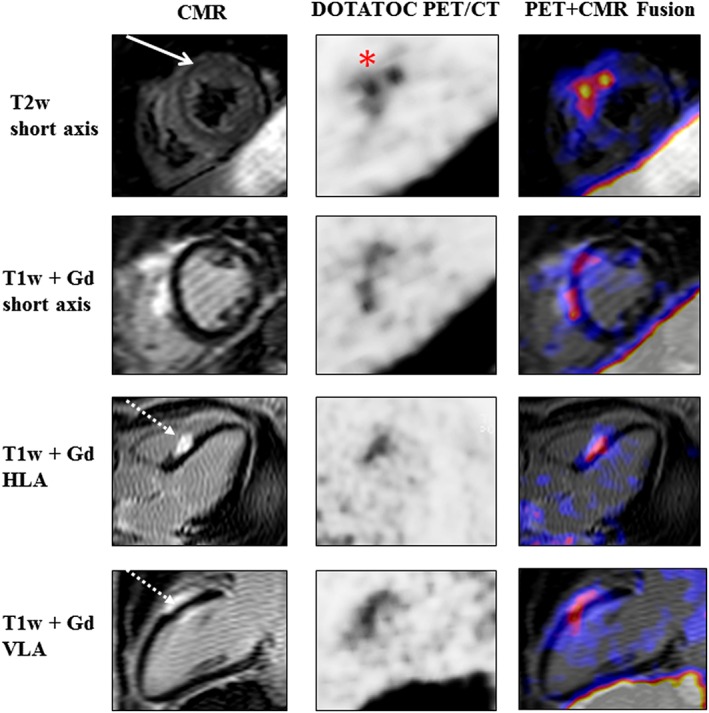
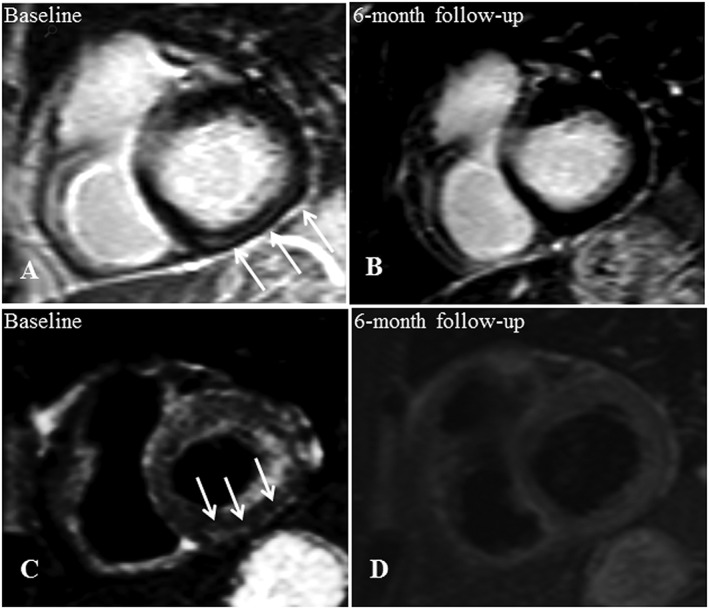
Methods and results: In a pilot study, we had previously identified cardiac involvement-diagnosed by CMR imaging-to be present in 29 of 188 patients (15.4%) with histologically proven, extra-CS. Out of these initial 29 CS-positive patients, 27 patients (49.9 ± 11.8 years, 59.3% male) were presently re-examined and underwent a second CMR study and complementary standard clinical testing. Somatostatin receptor scintigraphy using the ligand 68 Ga-DOTATOC was additionally performed when clinically indicated (17 patients). Within a median follow-up period of 2.6 years, none of the initial 29 patients deceased or experienced aborted sudden cardiac death. However, two patients developed third-degree atrioventricular block that required device therapy. Among the 27 re-examined CS patients, pathological CMR findings persisted in 14 of 27 patients (51.9%). CS remission was primarily due to a resolution of acute inflammatory processes. 68 Ga-DOTATOC positron emission tomography/computed tomography (PET/CT) identified one patient with regions of raised tracer uptake that concorded with acute inflammatory changes, as assessed by CMR; this patient received no immunosuppressive medication at the time of PET/CT execution.
Conclusions: Within follow-up, CS persisted in barely half the patients, and the patients were not afflicted with cardiac death. Additional 68 Ga-DOTATOC PET/CT allowed for visualization of acute myocardial inflammation.
Keywords: 68Ga-DOTATOC PET/CT; Cardiac sarcoidosis; Cardiovascular magnetic resonance.
© 2017 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures

References
-
- Statement on sarcoidosis. Joint Statement of the American Thoracic Society (ATS), the European Respiratory Society (ERS) and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG) adopted by the ATS Board of Directors and by the ERS Executive Committee, February 1999. Am J Respir Crit Care Med 1999; 160: 736–755. - PubMed
-
- Thomas KW, Hunninghake GW. Sarcoidosis. JAMA 2003; 289: 3300–3303. - PubMed
-
- Porterfield CP, Ferguson JD. Arrhythmia in cardiac sarcoidosis. J Cardiovasc Electrophysiol 2014; 25: 177–178. - PubMed
-
- Gideon NM, Mannino DM. Sarcoidosis mortality in the United States 1979–1991: an analysis of multiple‐cause mortality data. Am J Med 1996; 100: 423–427. - PubMed
-
- Iwai K, Tachibana T, Takemura T, Matsui Y, Kitaichi M, Kawabata Y. Pathological studies on sarcoidosis autopsy. I. Epidemiological features of 320 cases in Japan. Acta Pathol Jpn 1993; 43: 372–376. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
