

Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa: A mathematical modelling study
- PMID: 29232366
- PMCID: PMC5726614
- DOI: 10.1371/journal.pmed.1002468
Estimating the impact of antiretroviral treatment on adult mortality trends in South Africa: A mathematical modelling study
Abstract
Background: Substantial reductions in adult mortality have been observed in South Africa since the mid-2000s, but there has been no formal evaluation of how much of this decline is attributable to the scale-up of antiretroviral treatment (ART), as previous models have not been calibrated to vital registration data. We developed a deterministic mathematical model to simulate the mortality trends that would have been expected in the absence of ART, and with earlier introduction of ART.
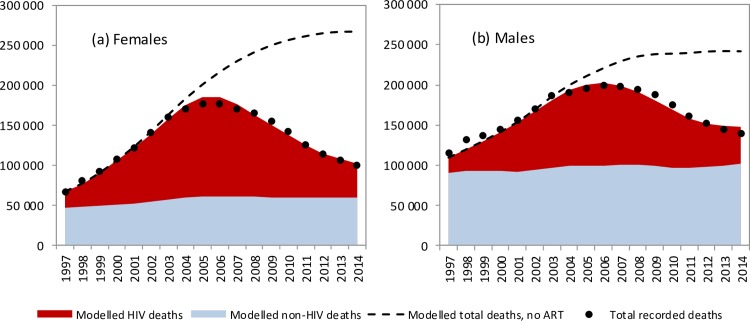
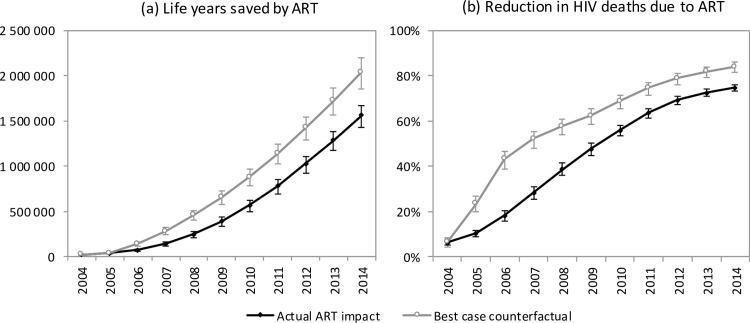
Methods and findings: Model estimates of mortality rates in ART patients were obtained from the International Epidemiology Databases to Evaluate AIDS-Southern Africa (IeDEA-SA) collaboration. The model was calibrated to HIV prevalence data (1997-2013) and mortality data from the South African vital registration system (1997-2014), using a Bayesian approach. In the 1985-2014 period, 2.70 million adult HIV-related deaths occurred in South Africa. Adult HIV deaths peaked at 231,000 per annum in 2006 and declined to 95,000 in 2014, a reduction of 74.7% (95% CI: 73.3%-76.1%) compared to the scenario without ART. However, HIV mortality in 2014 was estimated to be 69% (95% CI: 46%-97%) higher in 2014 (161,000) if the model was calibrated only to HIV prevalence data. In the 2000-2014 period, the South African ART programme is estimated to have reduced the cumulative number of HIV deaths in adults by 1.72 million (95% CI: 1.58 million-1.84 million) and to have saved 6.15 million life years in adults (95% CI: 5.52 million-6.69 million). This compares with a potential saving of 8.80 million (95% CI: 7.90 million-9.59 million) life years that might have been achieved if South Africa had moved swiftly to implement WHO guidelines (2004-2013) and had achieved high levels of ART uptake in HIV-diagnosed individuals from 2004 onwards. The model is limited by its reliance on all-cause mortality data, given the lack of reliable cause-of-death reporting, and also does not allow for changes over time in tuberculosis control programmes and ART effectiveness.
Conclusions: ART has had a dramatic impact on adult mortality in South Africa, but delays in the rollout of ART, especially in the early stages of the ART programme, have contributed to substantial loss of life. This is the first study to our knowledge to calibrate a model of ART impact to population-level recorded death data in Africa; models that are not calibrated to population-level death data may overestimate HIV-related mortality.
Conflict of interest statement
The authors have read the journal's policy and declare the following competing interests: MM received grants from the Newton Fund and the Worldwide Universities Network for a research visit to the University of Cape Town directly related to this work and also from the UK Medical Research Council (MRC) [grant number MR/J002380/1] and the UK Department for International Development (DFID) under the MRC/DFID Concordat agreement which is part of the EDCTP2 programme supported by the European Union for work on HIV prognosis in the last 5 years. ME receives a stipend as a specialty consulting editor for
Figures
Comment in
-
Antiretroviral therapy and population mortality: Leveraging routine national data to advance policy.PLoS Med. 2017 Dec 12;14(12):e1002469. doi: 10.1371/journal.pmed.1002469. eCollection 2017 Dec. PLoS Med. 2017. PMID: 29232374 Free PMC article.
References
-
- Statistics South Africa. Mortality and causes of death in South Africa, 2014: findings from death notification. Pretoria: Statistics South Africa; 2015. [cited 2016 Mar 13]. Available from: http://www.statssa.gov.za/publications/P03093/P030932014.pdf.
-
- Bradshaw D, Msemburi W, Dorrington R, Pillay-van Wyk V, Laubscher R, Groenewald P. HIV/AIDS in South Africa: how many people died from the disease between 1997 and 2010? AIDS. 2016;30:771–8. doi: 10.1097/QAD.0000000000000947 - DOI - PubMed
-
- Dorrington R, Bradshaw D, Laubscher R. Rapid mortality surveillance report 2012. Cape Town: South African Medical Research Council; 2014. [cited 2014 Apr 21]. Available from: http://www.mrc.ac.za/bod/RapidMortalitySurveillanceReport2012.pdf.
-
- Pillay-van Wyk V, Msemburi W, Laubscher R, Dorrington RE, Groenewald P, Glass T, et al. Mortality trends and differentials in South Africa from 1997 to 2012: second National Burden of Disease Study. Lancet Glob Health. 2016;4:e642–53. doi: 10.1016/S2214-109X(16)30113-9 - DOI - PubMed
-
- Reniers G, Slaymaker E, Nakiyingi-Miiro J, Nyamukapa C, Crampin AC, Herbst K, et al. Mortality trends in the era of antiretroviral therapy: evidence from the Network for Analysing Longitudinal Population based HIV/AIDS data on Africa (ALPHA). AIDS. 2014;28(Suppl 4):S533–42. doi: 10.1097/QAD.0000000000000496 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
